 Submit an article
Submit an article
Articles
- Page Path
- HOME > J Korean Acad Nurs > Volume 56(2); 2026 > Article
-
Review Paper
- Effectiveness of mobile health interventions to improve medication adherence for patients with cardiovascular disease: a systematic review and meta-analysis
-
Yeoungsuk Song1
 , Seurk Park2, Yuyoung Lee1, Sohye Lee3
, Seurk Park2, Yuyoung Lee1, Sohye Lee3 -
Journal of Korean Academy of Nursing 2026;56(2):148-165.
DOI: https://doi.org/10.4040/jkan.26016
Published online: May 22, 2026
1College of Nursing, Kyungpook National University, Daegu, South Korea
2School of Nursing, Gyeongkuk National University, Andong, South Korea
3Loewenberg College of Nursing, University of Memphis, Memphis, TN, USA
- Corresponding author: Seurk Park School of Nursing, Gyeongkuk National University, 1375 Gyeongdong-ro, Andong 36729, South Korea E-mail: ps@gknu.ac.kr
• Received: February 4, 2026 • Revised: April 19, 2026 • Accepted: April 22, 2026
© 2026 Korean Society of Nursing Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution NoDerivs License (http://creativecommons.org/licenses/by-nd/4.0) If the original work is properly cited and retained without any modification or reproduction, it can be used and re-distributed in any format and medium.
- 1,077 Views
- 84 Download
Abstract
-
Purpose
- This study systematically reviewed and synthesized the evidence on the effectiveness of mobile health (mHealth) interventions in improving medication adherence among patients with cardiovascular disease.
-
Methods
- This systematic review included randomized controlled trials that evaluated the effects of mHealth interventions on medication adherence among patients with cardiovascular disease. PubMed, the Cochrane Library, CINAHL, and Embase were searched for peer-reviewed studies and grey literature published in English between January 1, 2013, and July 31, 2025. The Cochrane Risk of Bias 2 (RoB 2) tool was used to assess the risk of bias in the included studies. R software ver. 4.5.2 was used to perform the meta-analysis.
-
Results
- Fifty-two studies were included in the systematic review, of which 20 were included in the meta-analysis. The pooled analysis demonstrated a significant improvement in medication adherence among patients with cardiovascular disease receiving mHealth interventions, with a moderate to large effect size (Hedges’ g=0.72; 95% confidence interval, 0.20–1.25; p<.001), despite substantial heterogeneity (I2=97%). However, a considerable proportion of the included studies were assessed as having a high risk of bias, which may limit the internal validity of the findings. Subgroup analyses indicated that the effects of mHealth interventions on medication adherence did not differ significantly according to intervention type, duration, or outcome measurement tools.
-
Conclusion
- mHealth interventions appear to be effective in improving medication adherence among patients with cardiovascular disease. However, these findings should be interpreted with caution because of the high risk of bias and substantial heterogeneity among the included studies. Future research should explore the use of emerging technologies, such as artificial intelligence and virtual reality, to address medication non-adherence (PROSPERO registration number: CRD42023450502).
Introduction
Methods
Results
1) Participant characteristics
2) Intervention characteristics
3) Comparator
4) Outcome measurement tools
1) Intervention effectiveness: medication adherence
2) Subgroup analysis
(1) Intervention type
(2) Intervention duration
(3) Outcome measurement tools
Discussion
Conclusion
-
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
-
Acknowledgements
None.
-
Funding
This research was supported by Kyungpook National University Research Fund, 2023.
-
Data Sharing Statement
Please contact the corresponding author for data availability.
-
Supplementary Data
Supplementary data to this article can be found online at https://doi.org/10.4040/jkan.26016.
Supplementary Appendix 1. Search strategy to identify relevant studies across databases
jkan-26016-Supplementary-Appendix-1.pdf
Supplementary Appendix 2. Included studies in systematic review
jkan-26016-Supplementary-Appendix-2.pdf
Supplementary Table 1. Results of subgroup analyses by intervention type, intervention duration, and outcome measurement tools
jkan-26016-Supplementary-Table-1.pdf
Supplementary Figure 1. Funnel plot
-
Author Contributions
Conceptualization: YS, SP, SL, YL. Data curation: YS, SP, SL, YL. Final approval of the manuscript: all authors. Formal analysis: YS, SP, SL, YL. Funding acquisition: YS. Investigation: YS. Methodology: YS, SP, SL, YL. Project administration: YS. Resources: SP, SL. Software: SP, SL. Supervision: YS. Validation: YS, SP, SL, YL. Visualization: SP, SL. Writing–original draft: YS, SP, SL, YL. Writing–review & editing: YS, SP, SL, YL.
Article Information
Fig. 1.PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) flow diagram of study selection for the systematic review and meta-analysis.
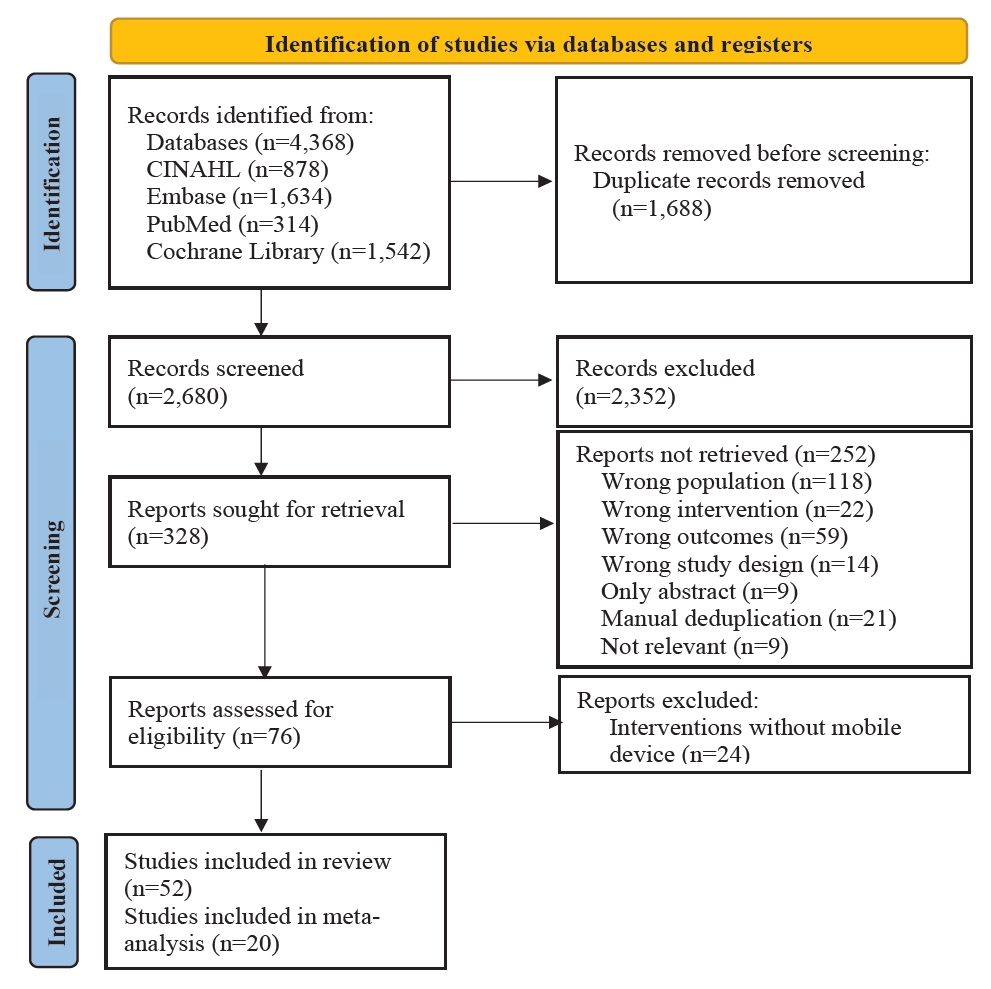
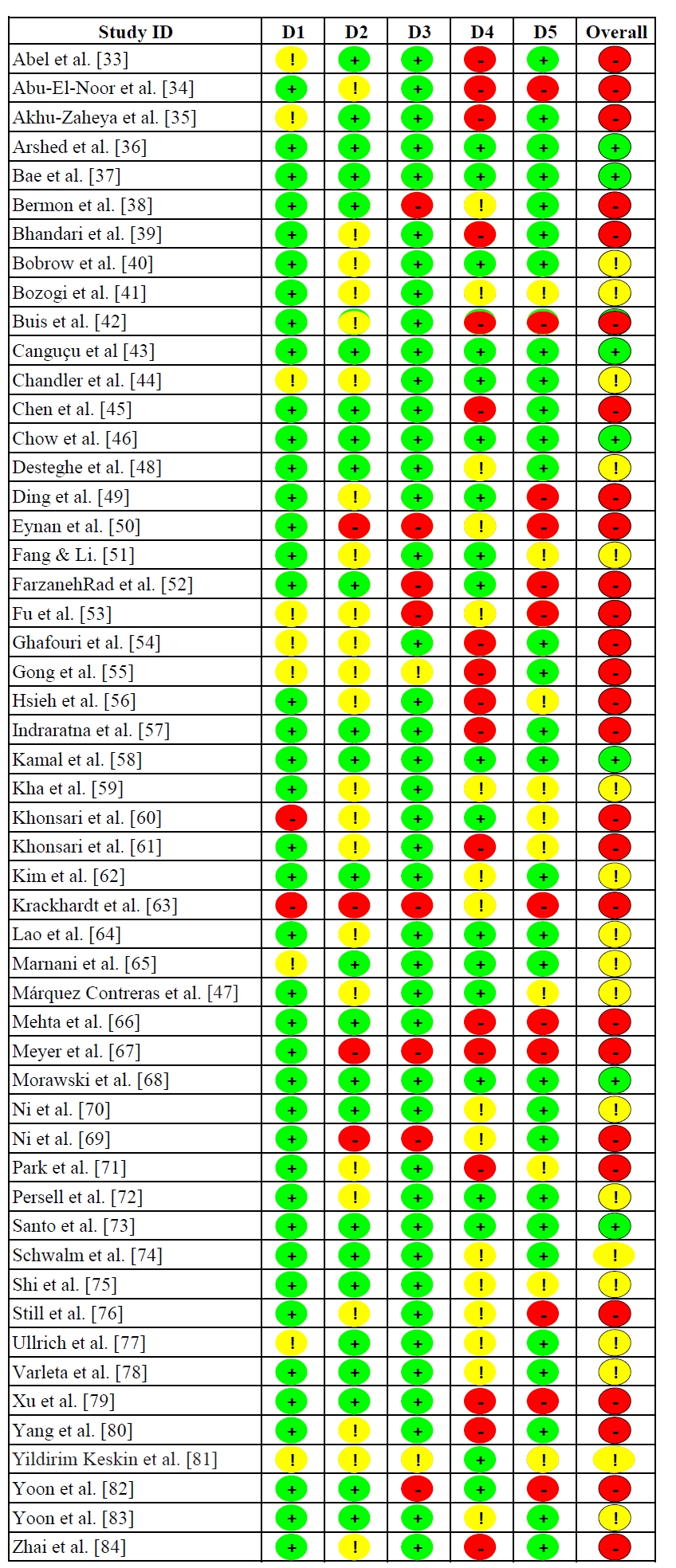
Fig. 3.Forest plot of the overall effect size of mHealth interventions on medication adherence in patients with cardiovascular disease. CI, confidence interval; SD, standard deviation; SMD, standardized mean difference.
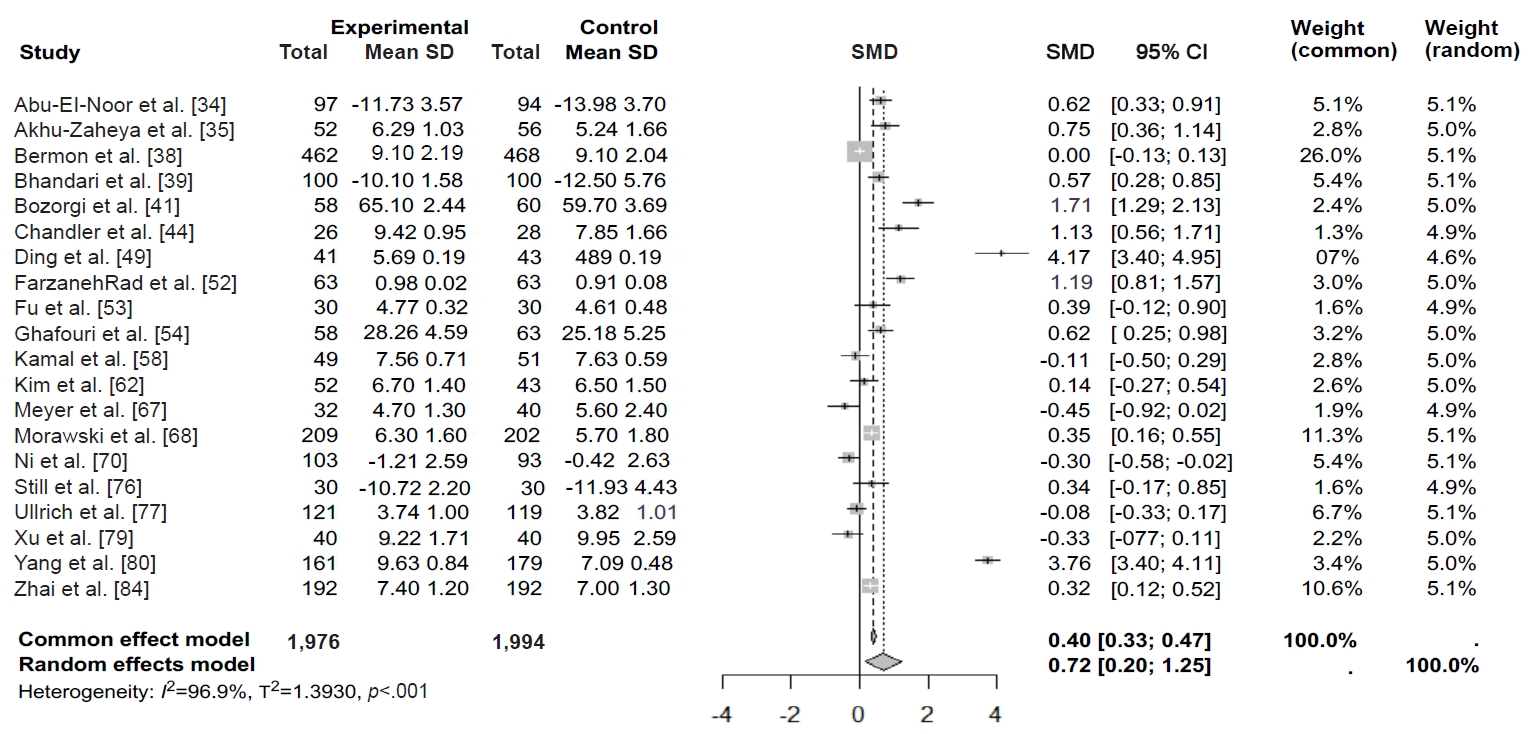
Table 1.Descriptive summary of the included studies (N=52)
CVD, cardiovascular disease; RCT, randomized controlled trial.
a)Other countries include Jordan, Pakistan, Colombia, Nepal, South Africa, Brazil, Spain, Belgium, Canada, Iran, Taiwan, Palestine, Malaysia, Germany, Chile, and Turkey, as well as one multinational study. b)Others include cluster RCTs, crossover RCTs, and mixed-methods RCTs. c)Mixed or general CVD includes general CVD and combined conditions such as acute coronary syndrome, heart failure, or mechanical valve replacement.
Table 2.Characteristics of studies included in the systematic review (N=52)
| Author (year), country | Study design | Participant/sample size | Intervention type | Duration (wk) | Comparator | Outcome measurement tools |
|---|---|---|---|---|---|---|
| Abel et al. [33] (2023), USA | Pilot RCT | Black women diagnosed with hypertension (N=77; EG=41, CG=36) | Interactive technology-enhanced coaching (wearable monitoring and coaching with integrated data tracking) | 36 | Active comparator | Self-reported MA |
| Abu-El-Noor et al. [34] (2021), Palestine | RCT | Patients with hypertension (N=191; EG=97, CG=94) | Mobile app with medication reminders, education, and BP self-monitoring | 12 | Usual care | HBCS |
| Akhu-Zaheya et al. [35] (2017), Jordan | RCT | Patients with CVD (N=160; EG=52, Placebo=52, CG=56) | SMS (adherence, diet, and smoking cessation) vs. general messages (placebo) | 12 | Usual care | MMAS-8 |
| Arshed et al. [36] (2024), Pakistan | RCT | Patients with hypertension (N=423; EG=214, CG=209) | Mobile app-based reminders and education | 24 | Standard care | Pill count |
| Bae et al. [37] (2021), South Korea | RCT | Older patients with CHD (N=879; EG=440, CG=439) | One-way SMS and website support | 24 | Standard care | MMS |
| Bermon et al. [38] (2021), Colombia | RCT | Patients with atherosclerotic CVD (N=930; EG=462, CG=468) | SMS (education and behavior change) | 52 | Active comparator | MMAS-8 |
| Bhandari et al. [39] (2022), Nepal | Pilot RCT | Patients with hypertension (N=200; EG=100, CG=100) | SMS (education, reminders, and tailored messages) | 12 | Standard care | HBCS |
| Bobrow et al. [40] (2016), South Africa | RCT | Adults with high BP (N=1,372; EG1=457, EG2=458, CG=457) | One-way SMS (EG1) vs. interactive SMS (EG2) | 52 | Usual care | PDC |
| Bozorgi et al. [41] (2021), Colombia | RCT | Patients with hypertension (N=120; EG=60, CG=60) | Mobile app for BP management | 8 | Usual care | HBCS |
| Buis et al. [42] (2024), USA | RCT | Patients with uncontrolled hypertension (N=87; EG=44, CG=43) | Mobile app with BP monitoring and pedometer | 48 | Usual care | ARMS-14 |
| Canguçu et al. [43] (2024), Brazil | Crossover RCT | Patients with hypertension (N=155; EG=77, CG=78) | Text messages with and without reminders | 12 | No intervention | BMQ |
| Chandler et al. [44] (2019), USA | RCT | Hispanic adults with uncontrolled hypertension (N=54; EG=26, CG=28) | Smartphone app with medication adherence stops hypertension | 36 | Active comparator | MMAS |
| Chen et al. [45] (2019), China | RCT | Patients with CHF (N=767; EG1=252, EG2=255, CG=260) | SMS (EG1) vs. structured telephone support (EG2) | 26 | Usual care | Self-reported MA |
| Chow et al. [46] (2022), Australia | RCT | Patients with ACS (N=95; EG=52, CG=43) | Text message-based cardiac education and support | 52 | Usual care | Self-reported MA |
| Márquez Contreras et al. [47] (2019), Spain | RCT | Participant with hypertension (N=154; EG=77, CG=77) | Smartphone app for hypertension management | 52 | Usual care | Electronic MEMS |
| Desteghe et al. [48] (2025), Belgium | RCT | Patients with AF (N=1,038; EG1=345, EG2=347, CG=346) | In-person education (EG1), online education (EG2) | 4,12,24,48 (every 24-wk until study end) | Standard care | Electronic MEMS |
| Ding et al. [49] (2024), China | RCT | Patients with mechanical valve replacement (N=84; EG=41, CG=43) | Mobile app for self-monitoring, medication reminders, and nurse-supported follow-up care | 24 | Standard care | MMAS-8 |
| Eynan et al. [50] (2024), Canada | Pilot study | Patients with CHF (N=54; EG1=14, EG2 =13, EG3=12, CG=15) | Text messages for education and medication reminders (EG1) vs. coaching (EG2) vs. combined intervention (EG3) | 12 | Usual care | MMAS-8 |
| Fang & Li [51] (2016), China | RCT | Outpatients with CAD (N=271; EG1=91, EG2=90 EG3=90) | SMS reminders and education material via SMS alone (EG1) vs. SMS and micro letter (EG2) vs. phone (EG3) | 24 | Active comparator | MMAS |
| FarzanehRad et al. [52] (2024), Iran | RCT | Patients with HF (N=159; EG1=50, EG2=54, CG=55) | Tailored text messaging (EG1) vs. pillbox organizers (EG2) | 12 | Usual care | MARS, pill count |
| Fu et al. [53] (2025), China | RCT | Patients with CHD (N=60; EG=30, CG=30) | Internet-based continuous nursing with multidisciplinary support | 24 | Standard care | MMAS |
| Ghafouri et al. [54] (2024), Iran | RCT | Persons with cardiac disease (N=121; EG=58, CG=63) | Mobile app with education, risk assessment, and feedback | 3 | Usual care | MAQ |
| Gong et al [55] (2020), China | RCT | Patients with hypertension (N=443; EG=225, CG=218) | Yan Fu app with self-monitoring, reminders, education, and alerts | 24 | Usual care | MMAS-8 |
| Hsieh et al. [56] (2021), Taiwan | RCT | Patients with AF (N=231; EG=115, CG=116) | Web-based integrated management with education, monitoring, and multidisciplinary support | 24 | Usual care | MARS |
| Indraratna et al. [57] (2022), Australia | Pilot RCT | Patients with ACS or HF (N=164; EG=81, CG=83) | TeleClinical Care smartphone app with telemonitoring and educational messaging | 28 | Usual care | MGL |
| Kamal et al. [58] (2018), Pakistan | RCT | Patients with CAD (N=100; EG=49, CG=51) | Interactive voice response-based tailored medication reminders and education | 12 | Usual care | MMAS-8 |
| Kha et al. [59] (2025), Australia | RCT | Patients with ACS (N=1,379; EG=697, CG=682) | SMS (medication adherence and lifestyle change) | 48 | Standard care | Self-reported adherence based on missed days |
| Khonsari et al. [60] (2015), Malaysia | Mixed-methods RCT | Patients with ACS (N=62; EG=31, CG=31) | Automated web-based system for SMS management | 8 | Usual care | MMAS-8 |
| Khonsari et al. [61] (2020), Iran | Mixed-methods RCT | Patients with CHD (N=78; EG=39, CG=39) | SMS medication reminders | 12 | Usual care | MMAS-8 |
| Kim et al. [62] (2016), USA | RCT | Patients with hypertension (N=95; EG=52, CG=43) | Wireless self-monitoring platform with app support and nurse monitoring | 24 | Standard care | MMAS-8 |
| Krackhardt et al. [63] (2023), Germany | RCT | Patients with ACS (N=676; EG=342, CG=334) | Smartphone app with reminders and motivational messages | 4 | No intervention | BAQ |
| Lao et al. [64] (2023), China | RCT | Patients with CHD (N=140; EG=70, CG=70) | Mobile health app for cardiac rehabilitation | 12 | Usual care | Pill count |
| Magnani et al. [65] (2025), USA | RCT | Patients with AF (N=243; EG=123, CG=120) | Smartphone app with a relational agent for education, adherence monitoring, self-care, and heart rate and rhythm monitoring | 48 | Active comparator | PDC |
| Mehta et al. [66] (2024), USA | RCT | Patients with hypertension (N=86; EG1=35, EG2=36, CG=15) | Bidirectional SMS monitoring | 12 | Usual care | Self-reported MA |
| Meyer et al. [67] (2025), Germany | RCT | Patients with hypertension (N=102; EG=52, CG=50) | Internet-based cognitive behavioral therapy, lifestyle counseling, and self-monitoring | 12 | Usual care | RAI |
| Morawski et al. [68] (2018), USA | RCT | Patients with uncontrolled hypertension (N=411; EG=209, CG=202) | Medisafe smartphone app | 12 | Usual care | MMAS-8 |
| Ni et al. [69] (2018), China | RCT | Patients with CHD (N=50; EG=25, CG=25) | Text messages (education via WeChat and medication reminders) | 4 | Usual care | VES |
| Ni et al. [70] (2022), China | RCT | Patients with CHD (N=196; EG=103, CG=93) | Messaging intervention (reminders and education) | 9 | Usual care | VES |
| Park et al. [71] (2015), USA | RCT | Patients with CHD (N=90; EG1=30, EG2=30, CG=30) | SMS reminders and education (EG1) vs. SMS (education only) | 4 | No intervention | MMAS-8 |
| Persell et al. [72] (2020), USA | RCT | Participant with uncontrolled hypertension (N=333; EG=166, CG=167) | Smartphone coaching app with home BP monitoring | 24 | Active comparator | Self-reported MA |
| Santo et al. [73] (2019), Australia | RCT | Patients with CHD (N=163; EG=107, CG=56) | Medication reminder smartphone apps | 12 | Usual care | MMAS-8 |
| Schwalm et al. [74] (2019), Colombia and Malaysia | Cluster RCT | Patients with hypertension (N=1,371; EG=740, CG=631) | Tablet-based management algorithm, counselling, and adherence support | 48 | Usual care | MMAS-8 |
| Shi et al. [75] (2025), China | RCT | Patients with AF (N=208, EG=104, CG=104) | Digital animation-based education | 12 | Standard care | MARS-5 |
| Still et al. [76] (2020), USA | RCT | African Americans with hypertension (N=60; EG=30, CG=30) | Community and technology-based hypertension self-management | 12 | Usual care | HBCS |
| Ullrich et al. [77] (2025), Germany | RCT | Patients with CAD (N=240; EG=121, CG=119) | PreventiPlaque app for lifestyle change and adherence support | 48 | Standard care | Self-assessment of MA |
| Varleta et al. [78] (2017), Chile | RCT | Patients with hypertension (N=314; EG=163, CG=151) | SMS (education for medication adherence) | 24 | No intervention | MGL |
| Xu et al. [79] (2024), China | RCT | Patients with AF (N=96; EG=48, CG=48) | Alfalfa app for comprehensive AF management | 12 | Standard care | MMAS-8 |
| Yang et al. [80] (2023), China | RCT | Patients with hypertension (N=368; EG=184, CG=184) | Transitional care with WeChat support, telephone follow-up, and home visits | 52 | Usual care | Self-designed questionnaire |
| Yildirim Keskin et al. [81] (2025), Turkey | RCT | Patients with hypertension (N=80; EG=40, CG=40) | Mobile app with self-monitoring, medication reminders, education, and feedback | 5 | Standard care | HBCS |
| Yoon et al. [82] (2024), South Korea | RCT | Patients with AF (N=498; EG=248, CG=250) | App-based feedback for edoxaban adherence support | 24 | Standard care | Pill count |
| Yoon et al. [83] (2025), South Korea | RCT | Patients with uncontrolled hypertension (N=154; EG=79, CG=75) | BP self-monitoring app with feedback | 24 | Active comparator | Pill count |
| Zhai et al. [84] (2020), China | Cluster RCT | Patients with hypertension (N=384; EG=192, CG=192) | SMS and personal consultation | 12 | Usual care | MMAS-8 |
ACS, acute coronary syndrome; AF, atrial fibrillation; Apps, applications; ARMS-14, adherence to refills and medication scale; BAQ, Brilique Adherence Questionnaire; BMQ, Brief Medication Questionnaire; BP, blood pressure; CAD, coronary artery disease; CG, control group; CHD, coronary heart disease; CHF, chronic heart failure; CVD, cardiovascular disease; EG, experimental group; HBCS, Hill-Bone Compliance Scale; HF, heart failure; MA, medication adherence; MAQ, Medication Adherence Questionnaire; MARS, Medication Adherence Rating Scale; MEMS, medication event monitoring system; MGL, Morisky-Green-Levine; MMAS, Morisky Medication Adherence Scale; MMAS-8, Morisky Medication Adherence Scale-8; MMS, Modified Morisky Scale; N, total sample size; PDC, proportion of days covered; RAI, Rief Adherence Index; RCT, randomized controlled trial; SMS, short message service; VES, Voils Medication Non-Adherence Extent Scale.
- 1. Statistics Korea. Cause of death statistics in 2024 [Internet]. Statistics Korea; 2025 [cited 2026 Jan 27]. Available from: https://www.kostat.go.kr/board.es?mid=a10301010000&bid=218
- 2. World Health Organization. The top 10 causes of death [Internet]. World Health Organization; 2024 [cited 2025 Dec 23]. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death
- 3. Woodruff RC, Tong X, Khan SS, Shah NS, Jackson SL, Loustalot F, et al. Trends in cardiovascular disease mortality rates and excess deaths, 2010-2022. Am J Prev Med. 2024;66(4):582-589. https://doi.org/10.1016/j.amepre.2023.11.009Article
- 4. Laflamme SZ, Bouchard K, Sztajerowska K, Lalande K, Greenman PS, Tulloch H. Attachment insecurities, caregiver burden, and psychological distress among partners of patients with heart disease. PLoS One. 2022;17(9):e0269366. https://doi.org/10.1371/journal.pone.0269366Article
- 5. McGreavy P. Managing mental well-being and the emotional aspects of cardiovascular disease: views from the patient lounge. Eur Heart J. 2023;44(15):1291-1292. https://doi.org/10.1093/eurheartj/ehac609ArticlePubMed
- 6. Mei S, Qin Z, Yang Y, Gao T, Ren H, Hu Y, et al. Influence of life satisfaction on quality of life: mediating roles of depression and anxiety among cardiovascular disease patients. Clin Nurs Res. 2021;30(2):215-224. https://doi.org/10.1177/1054773820947984Article
- 7. Javed Z, Haisum Maqsood M, Yahya T, Amin Z, Acquah I, Valero-Elizondo J, et al. Race, racism, and cardiovascular health: applying a social determinants of health framework to racial/ethnic disparities in cardiovascular disease. Circ Cardiovasc Qual Outcomes. 2022;15(1):e007917. https://doi.org/10.1161/CIRCOUTCOMES.121.007917ArticlePubMed
- 8. Lopez-Neyman SM, Davis K, Zohoori N, Broughton KS, Moore CE, Miketinas D. Racial disparities and prevalence of cardiovascular disease risk factors, cardiometabolic risk factors, and cardiovascular health metrics among US adults: NHANES 2011-2018. Sci Rep. 2022;12(1):19475. https://doi.org/10.1038/s41598-022-21878-xArticlePubMedPMC
- 9. Martin SS, Aday AW, Almarzooq ZI, Anderson CA, Arora P, Avery CL, et al. 2024 Heart disease and stroke statistics: a report of US and global data from the American Heart Association. Circulation. 2024;149(8):e347-e913. https://doi.org/10.1161/CIR.0000000000001209ArticlePubMedPMC
- 10. Cramer JA, Roy A, Burrell A, Fairchild CJ, Fuldeore MJ, Ollendorf DA, et al. Medication compliance and persistence: terminology and definitions. Value Health. 2008;11(1):44-47. https://doi.org/10.1111/j.1524-4733.2007.00213.xArticlePubMedPMC
- 11. American Heart Association. FACTS: a tough pill to swallow: medication adherence and cardiovascular disease fact sheet [Internet]. American Heart Association; 2021 [cited 2025 Jan 23]. Available from: https://www.heart.org/-/media/Files/About-Us/Policy-Research/Fact-Sheets/Access-to-Care/Medication-Adherence-and-CVD-Fact-Sheet.pdf?sc_lang=en
- 12. Hamrahian SM, Maarouf OH, Fülöp T. A critical review of medication adherence in hypertension: barriers and facilitators clinicians should consider. Patient Prefer Adherence. 2022;16:2749-2757. https://doi.org/10.2147/PPA.S368784ArticlePubMedPMC
- 13. Hennein R, Hwang SJ, Au R, Levy D, Muntner P, Fox CS, et al. Barriers to medication adherence and links to cardiovascular disease risk factor control: the Framingham Heart Study. Intern Med J. 2018;48(4):414-421. https://doi.org/10.1111/imj.13687ArticlePubMedPMC
- 14. Krishnamoorthy Y, Rajaa S, Rehman T, Thulasingam M. Patient and provider’s perspective on barriers and facilitators for medication adherence among adult patients with cardiovascular diseases and diabetes mellitus in India: a qualitative evidence synthesis. BMJ Open. 2022;12(3):e055226. https://doi.org/10.1136/bmjopen-2021-055226ArticlePubMedPMC
- 15. Simon ST, Kini V, Levy AE, Ho PM. Medication adherence in cardiovascular medicine. BMJ. 2021;374:n1493. https://doi.org/10.1136/bmj.n1493ArticlePubMed
- 16. Chen C, Li X, Su Y, You Z, Wan R, Hong K. Adherence with cardiovascular medications and the outcomes in patients with coronary arterial disease: “real-world” evidence. Clin Cardiol. 2022;45(12):1220-1228. https://doi.org/10.1002/clc.23898ArticlePubMedPMC
- 17. Du L, Cheng Z, Zhang Y, Li Y, Mei D. The impact of medication adherence on clinical outcomes of coronary artery disease: a meta-analysis. Eur J Prev Cardiol. 2017;24(9):962-970. https://doi.org/10.1177/2047487317695628ArticlePubMed
- 18. Livori AC, Dalli L, Nicholls SJ, Nelson AJ. Defining, measuring, and addressing medication non-adherence in cardiovascular disease. Future Cardiol. 2024;20(15-16):819-822. https://doi.org/10.1080/14796678.2024.2433888Article
- 19. Arshed M, Mahmud AB, Minhat HS, Ying LP, Umer MF. Effectiveness of mHealth interventions in medication adherence among patients with cardiovascular diseases: a systematic review. Diseases. 2023;11(1):41. https://doi.org/10.3390/diseases11010041ArticlePubMedPMC
- 20. Eaton C, Vallejo N, McDonald X, Wu J, Rodríguez R, Muthusamy N, et al. User engagement with mHealth interventions to promote treatment adherence and self-management in people with chronic health conditions: systematic review. J Med Internet Res. 2024;26:e50508. https://doi.org/10.2196/50508ArticlePubMedPMC
- 21. Pouls BP, Vriezekolk JE, Bekker CL, Linn AJ, van Onzenoort HA, Vervloet M, et al. Effect of interactive eHealth interventions on improving medication adherence in adults with long-term medication: systematic review. J Med Internet Res. 2021;23(1):e18901. https://doi.org/10.2196/18901ArticlePubMedPMC
- 22. National Institutes of Health. Mobile health: technology and outcomes in low and middle income countries (mHealth) [Internet]. National Institutes of Health; c2024 [cited 2025 Jun 13]. Available from: https://www.fic.nih.gov/Programs/Pages/mhealth.aspx
- 23. Li R, Liang N, Bu F, Hesketh T. The effectiveness of self-management of hypertension in adults using mobile health: systematic review and meta-analysis. JMIR Mhealth Uhealth. 2020;8(3):e17776. https://doi.org/10.2196/17776ArticlePubMedPMC
- 24. Liu S, Li J, Wan DY, Li R, Qu Z, Hu Y, et al. Effectiveness of eHealth self-management interventions in patients with heart failure: systematic review and meta-analysis. J Med Internet Res. 2022;24(9):e38697. https://doi.org/10.2196/38697ArticlePubMedPMC
- 25. Palmer MJ, Machiyama K, Woodd S, Gubijev A, Barnard S, Russell S, et al. Mobile phone-based interventions for improving adherence to medication prescribed for the primary prevention of cardiovascular disease in adults. Cochrane Database Syst Rev. 2021;3(3):CD012675. https://doi.org/10.1002/14651858.CD012675.pub3Article
- 26. Redfern J, Tu Q, Hyun K, Hollings MA, Hafiz N, Zwack C, et al. Mobile phone text messaging for medication adherence in secondary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2024;3(3):CD011851. https://doi.org/10.1002/14651858.CD011851.pub3ArticlePubMedPMC
- 27. Al-Arkee S, Mason J, Lane DA, Fabritz L, Chua W, Haque MS, et al. Mobile apps to improve medication adherence in cardiovascular disease: systematic review and meta-analysis. J Med Internet Res. 2021;23(5):e24190. https://doi.org/10.2196/24190ArticlePubMedPMC
- 28. Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160. https://doi.org/10.1136/bmj.n160ArticlePubMedPMC
- 29. Ali O, Abdelbaki W, Shrestha A, Elbasi E, Alryalat MA, Dwivedi YK. A systematic literature review of artificial intelligence in the healthcare sector: benefits, challenges, methodologies, and functionalities. J Innov Knowl. 2023;8(1):100333. https://doi.org/10.1016/j.jik.2023.100333Article
- 30. Clarivate Analytics. EndNote 20, version 20 [Internet]. Clarivate Analytics; 2022 [cited 2025 Jun 13]. Available from: https://endnote.com
- 31. Sterne JA, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. https://doi.org/10.1136/bmj.l4898ArticlePubMedPMC
- 32. Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions, version 6.5.0 [Internet]. The Cochrane Collaboration; 2024 [cited 2025 May 5]. Available from: https://www.cochrane.org/authors/handbooks-and-manuals/handbook
- 33. Abel WM, Efird JT, Crane PB, Ferdinand KC, Foy CG, DeHaven MJ. Use of coaching and technology to improve blood pressure control in Black women with hypertension: pilot randomized controlled trial study. J Clin Hypertens (Greenwich). 2023;25(1):95-105. https://doi.org/10.1111/jch.14617Article
- 34. Abu-El-Noor NI, Aljeesh YI, Bottcher B, Abu-El-Noor MK. Impact of a mobile phone app on adherence to treatment regimens among hypertensive patients: a randomised clinical trial study. Eur J Cardiovasc Nurs. 2021;20(5):428-435. https://doi.org/10.1177/1474515120938235ArticlePubMed
- 35. Akhu-Zaheya LM, Shiyab WY. The effect of short message system (SMS) reminder on adherence to a healthy diet, medication, and cessation of smoking among adult patients with cardiovascular diseases. Int J Med Inform. 2017;98:65-75. https://doi.org/10.1016/j.ijmedinf.2016.12.003ArticlePubMed
- 36. Arshed M, Mahmud A, Minhat HS, Lim PY, Zakar R. Effectiveness of a multifaceted mobile health intervention (multi-aid-package) in medication adherence and treatment outcomes among patients with hypertension in a low- to middle-income country: randomized controlled trial. JMIR Mhealth Uhealth. 2024;12:e50248. https://doi.org/10.2196/50248ArticlePubMedPMC
- 37. Bae JW, Woo SI, Lee J, Park SD, Kwon SW, Choi SH, et al. MHealth interventions for lifestyle and risk factor modification in coronary heart disease: randomized controlled trial. JMIR Mhealth Uhealth. 2021;9(9):e29928. https://doi.org/10.2196/29928ArticlePubMedPMC
- 38. Bermon A, Uribe AF, Pérez-Rivero PF, Prieto-Merino D, Saaibi JF, Silva FA, et al. Efficacy and safety of text messages targeting adherence to cardiovascular medications in secondary prevention: TXT2HEART Colombia Randomized Controlled Trial. JMIR Mhealth Uhealth. 2021;9(7):e25548. https://doi.org/10.2196/25548ArticlePubMedPMC
- 39. Bhandari B, Narasimhan P, Jayasuriya R, Vaidya A, Schutte AE. Effectiveness and acceptability of a mobile phone text messaging intervention to improve blood pressure control (TEXT4BP) among patients with hypertension in Nepal: a feasibility randomised controlled trial. Glob Heart. 2022;17(1):13. https://doi.org/10.5334/gh.1103Article
- 40. Bobrow K, Farmer AJ, Springer D, Shanyinde M, Yu LM, Brennan T, et al. Mobile phone text messages to support treatment adherence in adults with high blood pressure (SMS-Text Adherence Support [StAR]): a single-blind, randomized trial. Circulation. 2016;133(6):592-600. https://doi.org/10.1161/CIRCULATIONAHA.115.017530ArticlePubMedPMC
- 41. Bozorgi A, Hosseini H, Eftekhar H, Majdzadeh R, Yoonessi A, Ramezankhani A, et al. The effect of the mobile “blood pressure management application” on hypertension self-management enhancement: a randomized controlled trial. Trials. 2021;22(1):413. https://doi.org/10.1186/s13063-021-05270-0ArticlePubMedPMC
- 42. Buis LR, Kim J, Sen A, Chen D, Dawood K, Kadri R, et al. The effect of an mHealth self-monitoring intervention (MI-BP) on blood pressure among black individuals with uncontrolled hypertension: randomized controlled trial. JMIR Mhealth Uhealth. 2024;12:e57863. https://doi.org/10.2196/57863ArticlePubMedPMC
- 43. Canguçu E, Castro PR, Moreira PM, Bandeira P, Almeida K, Santos PM, et al. Use of text messages to promote medication adherence and reduce blood pressure in patients with hypertension: the ESSENCE study. Cad Saude Publica. 2024;40(11):e00050023. https://doi.org/10.1590/0102-311XEN050023ArticlePubMedPMC
- 44. Chandler J, Sox L, Kellam K, Feder L, Nemeth L, Treiber F. Impact of a culturally tailored mHealth medication regimen self-management program upon blood pressure among hypertensive Hispanic adults. Int J Environ Res Public Health. 2019;16(7):1226. https://doi.org/10.3390/ijerph16071226ArticlePubMedPMC
- 45. Chen C, Li X, Sun L, Cao S, Kang Y, Hong L, et al. Post-discharge short message service improves short-term clinical outcome and self-care behaviour in chronic heart failure. ESC Heart Fail. 2019;6(1):164-173. https://doi.org/10.1002/ehf2.12380Article
- 46. Chow CK, Klimis H, Thiagalingam A, Redfern J, Hillis GS, Brieger D, et al. Text messages to improve medication adherence and secondary prevention after acute coronary syndrome: the TEXTMEDS Randomized Clinical Trial. Circulation. 2022;145(19):1443-1455. https://doi.org/10.1161/CIRCULATIONAHA.121.056161ArticlePubMed
- 47. Márquez Contreras E, Márquez Rivero S, Rodríguez García E, López-García-Ramos L, Carlos Pastoriza Vilas J, Baldonedo Suárez A, et al. Specific hypertension smartphone application to improve medication adherence in hypertension: a cluster-randomized trial. Curr Med Res Opin. 2019;35(1):167-173. https://doi.org/10.1080/03007995.2018.1549026ArticlePubMed
- 48. Desteghe L, Delesie M, Knaepen L, Önder R, Verbeeck J, Dendale P, et al. Effect of targeted education of patients with atrial fibrillation on unplanned cardiovascular outcomes: results of the multicentre randomized AF-EduCare trial. Europace. 2024;27(1):euae211. https://doi.org/10.1093/europace/euae211ArticlePubMedPMC
- 49. Ding N, Luo X, Zhou J, Jiang X, Wang X. Intervention effect of the mobile phone APP based continuous care on patients after mechanical heart valve replacement: a randomised controlled trials. Rev Cardiovasc Med. 2024;25(9):314. https://doi.org/10.31083/j.rcm2509314Article
- 50. Eynan R, Petrella R, Forchuk C, Zwarenstein M, Calvin J. Randomised pilot study comparing a coach to SMARTPhone reminders to aid the management of heart failure (HF) patients: humans or machines. BMJ Open Qual. 2024;13(3):e002753. https://doi.org/10.1136/bmjoq-2024-002753Article
- 51. Fang R, Li X. Electronic messaging support service programs improve adherence to lipid-lowering therapy among outpatients with coronary artery disease: an exploratory randomised control study. J Clin Nurs. 2016;25(5-6):664-671. https://doi.org/10.1111/jocn.12988Article
- 52. FarzanehRad A, Allahbakhshian A, Gholizadeh L, Khalili AF, Hasankhani H. Randomized comparison of the effects of tailored text messaging versus pillbox organizers on medication adherence of heart failure patients. BMC Cardiovasc Disord. 2024;24(1):244. https://doi.org/10.1186/s12872-024-03884-1ArticlePubMedPMC
- 53. Fu H, Zhou G, Wang M, Chen Y. Research on Internet plus continuing nursing under dual heart medical model after percutaneous coronary intervention. Medicine (Baltimore). 2025;104(24):e42778. https://doi.org/10.1097/MD.0000000000042778ArticlePubMedPMC
- 54. Ghafouri R, Karbaschi R, Mashhadi Hosein A, Sharifian S. Development and efficacy of mobile application to improve medication adherence for persons with cardiac disease. ARYA Atheroscler. 2024;20(3):28-36. https://doi.org/10.48305/arya.2024.42169.2924Article
- 55. Gong K, Yan YL, Li Y, Du J, Wang J, Han Y, et al. Mobile health applications for the management of primary hypertension: a multicenter, randomized, controlled trial. Medicine (Baltimore). 2020;99(16):e19715. https://doi.org/10.1097/MD.0000000000019715ArticlePubMedPMC
- 56. Hsieh HL, Kao CW, Cheng SM, Chang YC. A web-based integrated management program for improving medication adherence and quality of life, and reducing readmission in patients with atrial fibrillation: randomized controlled trial. J Med Internet Res. 2021;23(9):e30107. https://doi.org/10.2196/30107Article
- 57. Indraratna P, Biswas U, McVeigh J, Mamo A, Magdy J, Vickers D, et al. A smartphone-based model of care to support patients with cardiac disease transitioning from hospital to the community (TeleClinical Care): pilot randomized controlled trial. JMIR Mhealth Uhealth. 2022;10(2):e32554. https://doi.org/10.2196/32554ArticlePubMedPMC
- 58. Kamal AK, Khalid W, Muqeet A, Jamil A, Farhat K, Gillani SR, et al. Making prescriptions “talk” to stroke and heart attack survivors to improve adherence: results of a randomized clinical trial (The Talking Rx Study). PLoS One. 2018;13(12):e0197671. https://doi.org/10.1371/journal.pone.0197671ArticlePubMedPMC
- 59. Kha R, Min H, Marschner S, Mahendran S, Thiagalingam A, Poulter R, et al. Determinants of medication adherence in patients with acute coronary syndrome: a secondary analysis of a randomised clinical trial. Heart. 2025;111(10):462-470. https://doi.org/10.1136/heartjnl-2024-325144ArticlePubMed
- 60. Khonsari S, Subramanian P, Chinna K, Latif LA, Ling LW, Gholami O. Effect of a reminder system using an automated short message service on medication adherence following acute coronary syndrome. Eur J Cardiovasc Nurs. 2015;14(2):170-179. https://doi.org/10.1177/1474515114521910Article
- 61. Khonsari S, Chandler C, Parker R, Holloway A. Increasing cardiovascular medication adherence: a Medical Research Council complex mHealth intervention mixed-methods feasibility study to inform global practice. J Adv Nurs. 2020;76(10):2670-2684. https://doi.org/10.1111/jan.14465Article
- 62. Kim JY, Wineinger NE, Steinhubl SR. The influence of wireless self-monitoring program on the relationship between patient activation and health behaviors, medication adherence, and blood pressure levels in hypertensive patients: a substudy of a randomized controlled trial. J Med Internet Res. 2016;18(6):e116. https://doi.org/10.2196/jmir.5429ArticlePubMedPMC
- 63. Krackhardt F, Jörnten-Karlsson M, Waliszewski M, Knutsson M, Niklasson A, Appel KF, et al. Results from the “Me & My Heart” (eMocial) Study: a randomized evaluation of a new smartphone-based support tool to increase therapy adherence of patients with acute coronary syndrome. Cardiovasc Drugs Ther. 2023;37(4):729-741. https://doi.org/10.1007/s10557-022-07331-1Article
- 64. Lao SS, Chair SY, Wang Q, Leong ML. The feasibility and effects of smartphone-based application on cardiac rehabilitation for patients after percutaneous coronary intervention: a randomized controlled trial. J Cardiovasc Nurs. 2024;39(1):88-101. https://doi.org/10.1097/JCN.0000000000000993Article
- 65. Magnani JW, Lalama CM, Abebe KZ, Ferry D, Rollman BL, Lancet MQ, et al. A mobile relational agent to enhance atrial fibrillation self-care: primary and secondary outcomes of a randomized controlled trial. Am Heart J. 2025;290:115-128. https://doi.org/10.1016/j.ahj.2025.06.009ArticlePubMed
- 66. Mehta SJ, Volpp KG, Troxel AB, Teel J, Reitz CR, Purcell A, et al. Remote blood pressure monitoring with social support for patients with hypertension: a randomized clinical trial. JAMA Netw Open. 2024;7(6):e2413515. https://doi.org/10.1001/jamanetworkopen.2024.13515ArticlePubMedPMC
- 67. Meyer B, Riepenhausen A, Betz LT, Jauch-Chara K, Reshetnik A. Internet-based digital intervention to support the self-management of hypertension compared to usual care: results of the HALCYON randomized controlled trial. BMC Cardiovasc Disord. 2025;25(1):256. https://doi.org/10.1186/s12872-025-04698-5ArticlePubMedPMC
- 68. Morawski K, Ghazinouri R, Krumme A, Lauffenburger JC, Lu Z, Durfee E, et al. Association of a smartphone application with medication adherence and blood pressure control: the MedISAFE-BP Randomized Clinical Trial. JAMA Intern Med. 2018;178(6):802-809. https://doi.org/10.1001/jamainternmed.2018.0447Article
- 69. Ni Z, Liu C, Wu B, Yang Q, Douglas C, Shaw RJ. An mHealth intervention to improve medication adherence among patients with coronary heart disease in China: development of an intervention. Int J Nurs Sci. 2018;5(4):322-330. https://doi.org/10.1016/j.ijnss.2018.09.003Article
- 70. Ni Z, Wu B, Yang Q, Yan LL, Liu C, Shaw RJ. An mHealth intervention to improve medication adherence and health outcomes among patients with coronary heart disease: randomized controlled trial. J Med Internet Res. 2022;24(3):e27202. https://doi.org/10.2196/27202ArticlePubMedPMC
- 71. Park LG, Howie-Esquivel J, Whooley MA, Dracup K. Psychosocial factors and medication adherence among patients with coronary heart disease: a text messaging intervention. Eur J Cardiovasc Nurs. 2015;14(3):264-273. https://doi.org/10.1177/1474515114537024ArticlePubMed
- 72. Persell SD, Peprah YA, Lipiszko D, Lee JY, Li JJ, Ciolino JD, et al. Effect of home blood pressure monitoring via a smartphone hypertension coaching application or tracking application on adults with uncontrolled hypertension: a randomized clinical trial. JAMA Netw Open. 2020;3(3):e200255. https://doi.org/10.1001/jamanetworkopen.2020.0255ArticlePubMedPMC
- 73. Santo K, Singleton A, Rogers K, Thiagalingam A, Chalmers J, Chow CK, et al. Medication reminder applications to improve adherence in coronary heart disease: a randomised clinical trial. Heart. 2019;105(4):323-329. https://doi.org/10.1136/heartjnl-2018-313479ArticlePubMed
- 74. Schwalm JD, McCready T, Lopez-Jaramillo P, Yusoff K, Attaran A, Lamelas P, et al. A community-based comprehensive intervention to reduce cardiovascular risk in hypertension (HOPE 4): a cluster-randomised controlled trial. Lancet. 2019;394(10205):1231-1242. https://doi.org/10.1016/S0140-6736(19)31949-XArticlePubMed
- 75. Shi X, Wang Y, Wang Y, Wang J, Peng C, Cheng S, et al. The effectiveness of digital animation-based multistage education for patients with atrial fibrillation catheter ablation: randomized clinical trial. J Med Internet Res. 2025;27:e65685. https://doi.org/10.2196/65685ArticlePubMedPMC
- 76. Still CH, Margevicius S, Harwell C, Huang MC, Martin L, Dang PB, et al. A community and technology-based approach for hypertension self-management (COACHMAN) to improve blood pressure control in African Americans: results from a pilot study. Patient Prefer Adherence. 2020;14:2301-2313. https://doi.org/10.2147/PPA.S283086ArticlePubMedPMC
- 77. Ullrich G, Bäuerle A, Jahre LM, Paldán K, Rosemeyer J, Kalaitzidis C, et al. Impact of visual presentation of atherosclerotic carotid plaque on cardiovascular risk profile using mHealth technologies. NPJ Digit Med. 2025;8(1):47. https://doi.org/10.1038/s41746-024-01423-yArticlePubMedPMC
- 78. Varleta P, Acevedo M, Akel C, Salinas C, Navarrete C, García A, et al. Mobile phone text messaging improves antihypertensive drug adherence in the community. J Clin Hypertens (Greenwich). 2017;19(12):1276-1284. https://doi.org/10.1111/jch.13098ArticlePubMedPMC
- 79. Xu W, Huang X, Lin Q, Wu T, Guan C, Lv M, et al. Application of Alfalfa App in the management of oral anticoagulation in patients with atrial fibrillation: a multicenter randomized controlled trial. BMC Med Inform Decis Mak. 2024;24(1):294. https://doi.org/10.1186/s12911-024-02701-1ArticlePubMedPMC
- 80. Yang R, Xu Y, Hou W, Wang L, Xiao S, Li C, et al. Transitional care for patients with portal hypertension: a multicenter study of intervention for post-TIPS patients. Clin Nurs Res. 2023;32(4):785-796. https://doi.org/10.1177/10547738221112746ArticlePubMed
- 81. Yildirim Keskin A, Özpancar Şolpan N, Değirmenci H. The effect of mobile application follow-up on treatment compliance and self-care management in patients with hypertension: randomized controlled trial. Public Health Nurs. 2025;42(1):275-285. https://doi.org/10.1111/phn.13476ArticlePubMed
- 82. Yoon M, Lee JH, Kim IC, Lee JH, Kim MN, Kim HL, et al. Smartphone app for improving self-awareness of adherence to edoxaban treatment in patients with atrial fibrillation (ADHERE-App Trial): randomized controlled trial. J Med Internet Res. 2024;26:e65010. https://doi.org/10.2196/65010ArticlePubMedPMC
- 83. Yoon M, Hur T, Park SJ, Jo SH, Kim EJ, Kim SJ, et al. Self-monitoring of blood pressure and feedback via mobile app in treatment of uncontrolled hypertension: the SMART-BP Randomized Clinical Trial. Mayo Clin Proc. 2025;100(5):840-853. https://doi.org/10.1016/j.mayocp.2024.09.018ArticlePubMed
- 84. Zhai P, Hayat K, Ji W, Li Q, Shi L, Atif N, et al. Efficacy of text messaging and personal consultation by pharmacy students among adults with hypertension: randomized controlled trial. J Med Internet Res. 2020;22(5):e16019. https://doi.org/10.2196/16019ArticlePubMedPMC
- 85. Park LG, Ng F, Handley MA. The use of the Capability-Opportunity- Motivation Behavior (COM-B) model to identify barriers to medication adherence and the application of mobile health technology in adults with coronary heart disease: a qualitative study. PEC Innov. 2023;3:100209. https://doi.org/10.1016/j.pecinn.2023.100209ArticlePubMedPMC
- 86. de Oliveira-Filho AD, Morisky DE, Neves SJ, Costa FA, de Lyra DP. The 8-item Morisky Medication Adherence Scale: validation of a Brazilian-Portuguese version in hypertensive adults. Res Social Adm Pharm. 2014;10(3):554-561. https://doi.org/10.1016/j.sapharm.2013.10.006ArticlePubMed
- 87. Morisky Medication Adherence Scales (MMAS) [Internet]. Moriskyscale.com; 2025 [cited 2025 Oct 23]. Available from: https://www.moriskyscale.com/
- 88. Zhou L, Cheng K, Chen L, Hou X, Wan J. Effectiveness of eHealth for medication adherence in renal transplant recipients: systematic review and meta-analysis. J Med Internet Res. 2025;27:e73520. https://doi.org/10.2196/73520Article
- 89. Jeminiwa R, Hohmann L, Qian J, Garza K, Hansen R, Fox BI. Impact of eHealth on medication adherence among patients with asthma: a systematic review and meta-analysis. Respir Med. 2019;149:59-68. https://doi.org/10.1016/j.rmed.2019.02.011ArticlePubMed
- 90. Kim MT, Hill MN, Bone LR, Levine DM. Development and testing of the Hill-Bone Compliance to High Blood Pressure Therapy Scale. Prog Cardiovasc Nurs. 2000;15(3):90-96. https://doi.org/10.1111/j.1751-7117.2000.tb00211.xArticlePubMedPMC
- 91. Machado B, Quimbaya P, Bustos RH, Jaimes D, Cortes K, Vargas D, et al. Assessment of medication adherence using mobile applications in chronic obstructive pulmonary disease: a scoping review. Int J Environ Res Public Health. 2024;21(10):1265. https://doi.org/10.3390/ijerph21101265ArticlePubMedPMC
- 92. López-Pineda A, Martinez-Muñoz M, Nouni-García R, Esquerdo-Arroyo A, Carbonell-Soliva Á, Ramirez-Familia E, et al. Methods and validity indicators for measuring adherence to statins in secondary cardiovascular prevention: a systematic review. Syst Rev. 2025;14(1):110. https://doi.org/10.1186/s13643-025-02853-9ArticlePubMedPMC
- 93. Schwarz A, Winkens LH, de Vet E, Ossendrijver D, Bouwsema K, Simons M. Design features associated with engagement in mobile health physical activity interventions among youth: systematic review of qualitative and quantitative studies. JMIR Mhealth Uhealth. 2023;11:e40898. https://doi.org/10.2196/40898ArticlePubMedPMC
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
Cite- Figure
-
- We recommend
- Related articles
-
- Variables influencing digital health literacy in older adults: a systematic review and meta-analysis
- Risk factors for the readmission of patients with diabetic ketoacidosis: a systematic review and meta-analysis
- Effectiveness of non-pharmacological interventions to reduce internalized stigma in people with severe mental illness: a systematic review and meta-analysis
- Effects of Non-Pharmacological Interventions on Major Adverse Cardiac Events in Patients Underwent Percutaneous Coronary Intervention: Systematic Review and Meta-Analysis
Effectiveness of mobile health interventions to improve medication adherence for patients with cardiovascular disease: a systematic review and meta-analysis
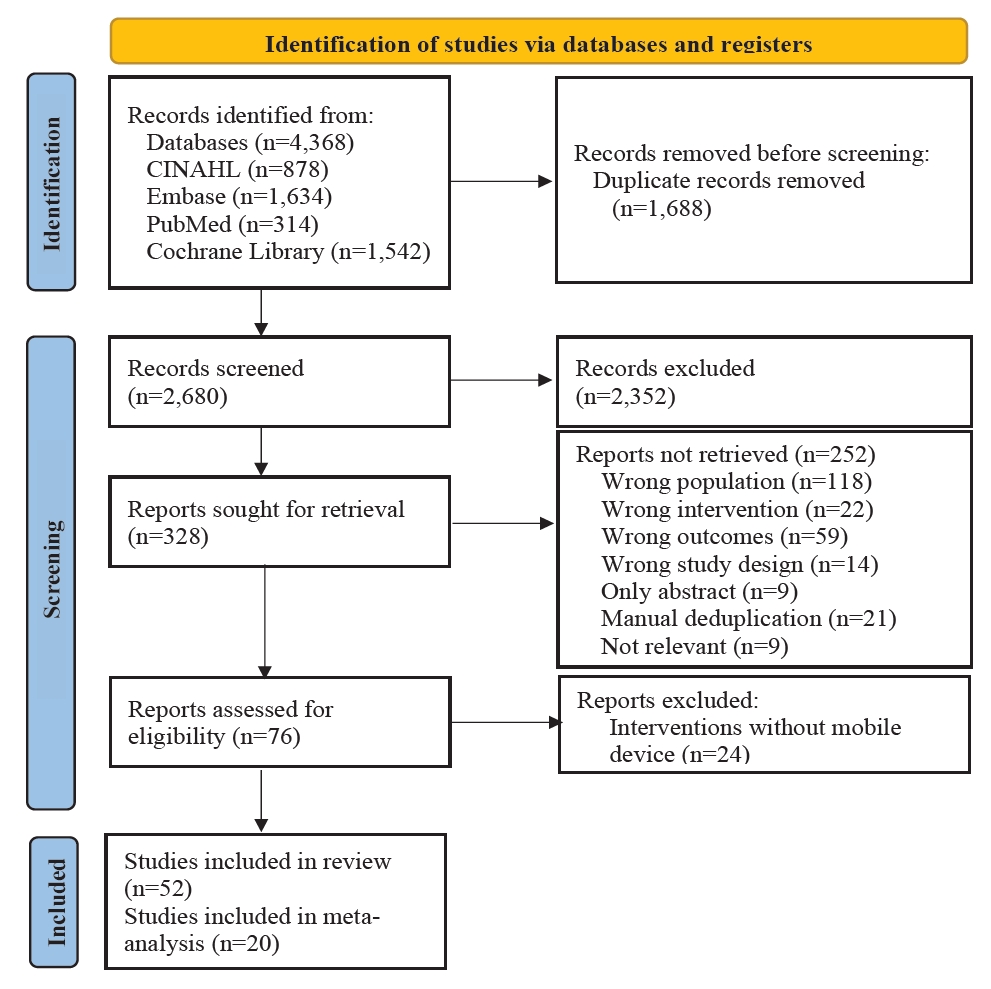
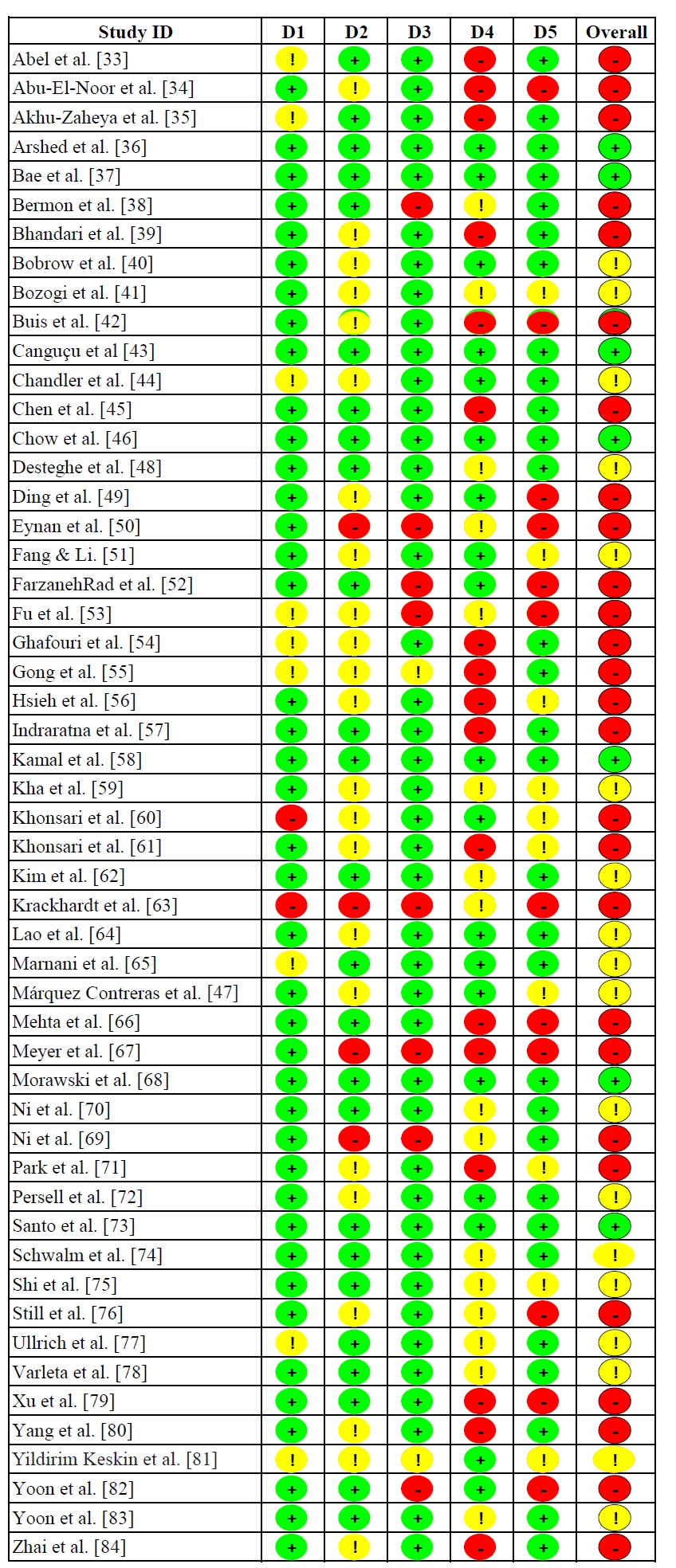
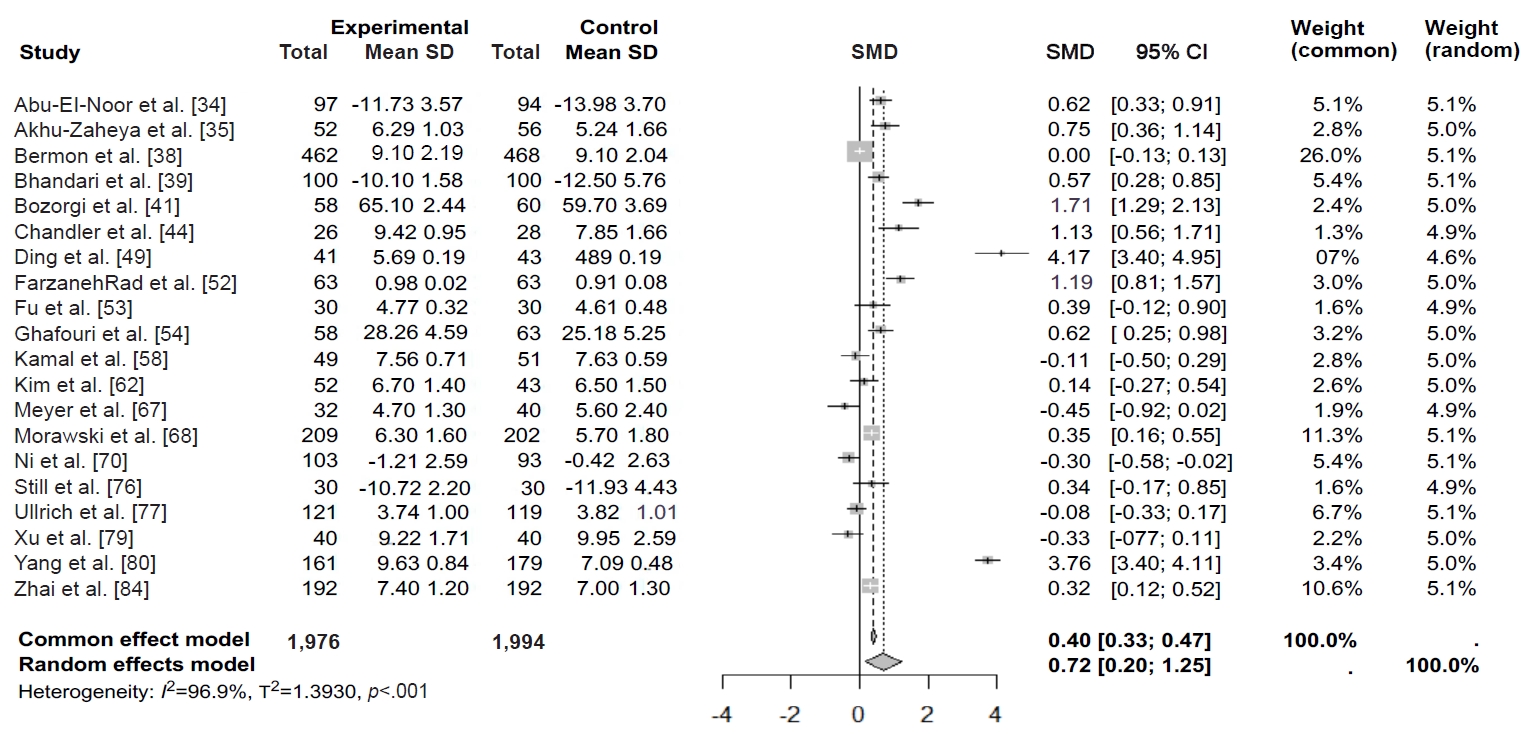
Fig. 1. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) flow diagram of study selection for the systematic review and meta-analysis.
Fig. 2. Risk of bias assessment of included studies.
Fig. 3. Forest plot of the overall effect size of mHealth interventions on medication adherence in patients with cardiovascular disease. CI, confidence interval; SD, standard deviation; SMD, standardized mean difference.
Fig. 1.
Fig. 2.
Fig. 3.
Effectiveness of mobile health interventions to improve medication adherence for patients with cardiovascular disease: a systematic review and meta-analysis
| Characteristic | Category | n (%) |
|---|---|---|
| Publication year | 2015–2019 | 15 (28.8) |
| 2020–2025 | 37 (71.2) | |
| Publication country | China | 12 (23.1) |
| USA | 10 (19.2) | |
| Australia | 4 (7.7) | |
| South Korea | 3 (5.8) | |
| Other countriesa) | 23 (44.2) | |
| Study design | RCT | 43 (82.7) |
| Pilot RCT | 4 (7.7) | |
| Othersb) | 5 (9.6) | |
| Participants | Hypertension | 23 (44.2) |
| Coronary heart disease | 8 (15.4) | |
| Atrial fibrillation | 6 (11.5) | |
| Acute coronary syndrome | 4 (7.7) | |
| Coronary artery disease | 3 (5.8) | |
| Heart failure | 3 (5.8) | |
| Mixed or general CVDc) | 5 (9.6) | |
| Sample size | <100 | 16 (30.8) |
| 100–299 | 20 (38.4) | |
| 300–999 | 12 (23.1) | |
| ≥1,000 | 4 (7.7) | |
| Type of intervention | Text message-based interventions | 20 (38.5) |
| Smartphone application-based interventions | 22 (42.3) | |
| Multicomponent mHealth interventions | 10 (19.2) | |
| Duration of intervention (wk) | ≤12 | 25 (48.1) |
| 13–24 | 12 (23.1) | |
| ≥25 | 15 (28.8) | |
| Comparator | Usual or standard care | 41 (78.8) |
| Active comparator | 7 (13.5) | |
| No intervention | 4 (7.7) | |
| Outcome measurement tools | Morisky-based tools | 22 (42.3) |
| Hill-Bone Compliance Scale | 5 (9.6) | |
| Other self-reported scales | 16 (30.8) | |
| Objective measures | 9 (17.3) |
| Author (year), country | Study design | Participant/sample size | Intervention type | Duration (wk) | Comparator | Outcome measurement tools |
|---|---|---|---|---|---|---|
| Abel et al. [33] (2023), USA | Pilot RCT | Black women diagnosed with hypertension (N=77; EG=41, CG=36) | Interactive technology-enhanced coaching (wearable monitoring and coaching with integrated data tracking) | 36 | Active comparator | Self-reported MA |
| Abu-El-Noor et al. [34] (2021), Palestine | RCT | Patients with hypertension (N=191; EG=97, CG=94) | Mobile app with medication reminders, education, and BP self-monitoring | 12 | Usual care | HBCS |
| Akhu-Zaheya et al. [35] (2017), Jordan | RCT | Patients with CVD (N=160; EG=52, Placebo=52, CG=56) | SMS (adherence, diet, and smoking cessation) vs. general messages (placebo) | 12 | Usual care | MMAS-8 |
| Arshed et al. [36] (2024), Pakistan | RCT | Patients with hypertension (N=423; EG=214, CG=209) | Mobile app-based reminders and education | 24 | Standard care | Pill count |
| Bae et al. [37] (2021), South Korea | RCT | Older patients with CHD (N=879; EG=440, CG=439) | One-way SMS and website support | 24 | Standard care | MMS |
| Bermon et al. [38] (2021), Colombia | RCT | Patients with atherosclerotic CVD (N=930; EG=462, CG=468) | SMS (education and behavior change) | 52 | Active comparator | MMAS-8 |
| Bhandari et al. [39] (2022), Nepal | Pilot RCT | Patients with hypertension (N=200; EG=100, CG=100) | SMS (education, reminders, and tailored messages) | 12 | Standard care | HBCS |
| Bobrow et al. [40] (2016), South Africa | RCT | Adults with high BP (N=1,372; EG1=457, EG2=458, CG=457) | One-way SMS (EG1) vs. interactive SMS (EG2) | 52 | Usual care | PDC |
| Bozorgi et al. [41] (2021), Colombia | RCT | Patients with hypertension (N=120; EG=60, CG=60) | Mobile app for BP management | 8 | Usual care | HBCS |
| Buis et al. [42] (2024), USA | RCT | Patients with uncontrolled hypertension (N=87; EG=44, CG=43) | Mobile app with BP monitoring and pedometer | 48 | Usual care | ARMS-14 |
| Canguçu et al. [43] (2024), Brazil | Crossover RCT | Patients with hypertension (N=155; EG=77, CG=78) | Text messages with and without reminders | 12 | No intervention | BMQ |
| Chandler et al. [44] (2019), USA | RCT | Hispanic adults with uncontrolled hypertension (N=54; EG=26, CG=28) | Smartphone app with medication adherence stops hypertension | 36 | Active comparator | MMAS |
| Chen et al. [45] (2019), China | RCT | Patients with CHF (N=767; EG1=252, EG2=255, CG=260) | SMS (EG1) vs. structured telephone support (EG2) | 26 | Usual care | Self-reported MA |
| Chow et al. [46] (2022), Australia | RCT | Patients with ACS (N=95; EG=52, CG=43) | Text message-based cardiac education and support | 52 | Usual care | Self-reported MA |
| Márquez Contreras et al. [47] (2019), Spain | RCT | Participant with hypertension (N=154; EG=77, CG=77) | Smartphone app for hypertension management | 52 | Usual care | Electronic MEMS |
| Desteghe et al. [48] (2025), Belgium | RCT | Patients with AF (N=1,038; EG1=345, EG2=347, CG=346) | In-person education (EG1), online education (EG2) | 4,12,24,48 (every 24-wk until study end) | Standard care | Electronic MEMS |
| Ding et al. [49] (2024), China | RCT | Patients with mechanical valve replacement (N=84; EG=41, CG=43) | Mobile app for self-monitoring, medication reminders, and nurse-supported follow-up care | 24 | Standard care | MMAS-8 |
| Eynan et al. [50] (2024), Canada | Pilot study | Patients with CHF (N=54; EG1=14, EG2 =13, EG3=12, CG=15) | Text messages for education and medication reminders (EG1) vs. coaching (EG2) vs. combined intervention (EG3) | 12 | Usual care | MMAS-8 |
| Fang & Li [51] (2016), China | RCT | Outpatients with CAD (N=271; EG1=91, EG2=90 EG3=90) | SMS reminders and education material via SMS alone (EG1) vs. SMS and micro letter (EG2) vs. phone (EG3) | 24 | Active comparator | MMAS |
| FarzanehRad et al. [52] (2024), Iran | RCT | Patients with HF (N=159; EG1=50, EG2=54, CG=55) | Tailored text messaging (EG1) vs. pillbox organizers (EG2) | 12 | Usual care | MARS, pill count |
| Fu et al. [53] (2025), China | RCT | Patients with CHD (N=60; EG=30, CG=30) | Internet-based continuous nursing with multidisciplinary support | 24 | Standard care | MMAS |
| Ghafouri et al. [54] (2024), Iran | RCT | Persons with cardiac disease (N=121; EG=58, CG=63) | Mobile app with education, risk assessment, and feedback | 3 | Usual care | MAQ |
| Gong et al [55] (2020), China | RCT | Patients with hypertension (N=443; EG=225, CG=218) | Yan Fu app with self-monitoring, reminders, education, and alerts | 24 | Usual care | MMAS-8 |
| Hsieh et al. [56] (2021), Taiwan | RCT | Patients with AF (N=231; EG=115, CG=116) | Web-based integrated management with education, monitoring, and multidisciplinary support | 24 | Usual care | MARS |
| Indraratna et al. [57] (2022), Australia | Pilot RCT | Patients with ACS or HF (N=164; EG=81, CG=83) | TeleClinical Care smartphone app with telemonitoring and educational messaging | 28 | Usual care | MGL |
| Kamal et al. [58] (2018), Pakistan | RCT | Patients with CAD (N=100; EG=49, CG=51) | Interactive voice response-based tailored medication reminders and education | 12 | Usual care | MMAS-8 |
| Kha et al. [59] (2025), Australia | RCT | Patients with ACS (N=1,379; EG=697, CG=682) | SMS (medication adherence and lifestyle change) | 48 | Standard care | Self-reported adherence based on missed days |
| Khonsari et al. [60] (2015), Malaysia | Mixed-methods RCT | Patients with ACS (N=62; EG=31, CG=31) | Automated web-based system for SMS management | 8 | Usual care | MMAS-8 |
| Khonsari et al. [61] (2020), Iran | Mixed-methods RCT | Patients with CHD (N=78; EG=39, CG=39) | SMS medication reminders | 12 | Usual care | MMAS-8 |
| Kim et al. [62] (2016), USA | RCT | Patients with hypertension (N=95; EG=52, CG=43) | Wireless self-monitoring platform with app support and nurse monitoring | 24 | Standard care | MMAS-8 |
| Krackhardt et al. [63] (2023), Germany | RCT | Patients with ACS (N=676; EG=342, CG=334) | Smartphone app with reminders and motivational messages | 4 | No intervention | BAQ |
| Lao et al. [64] (2023), China | RCT | Patients with CHD (N=140; EG=70, CG=70) | Mobile health app for cardiac rehabilitation | 12 | Usual care | Pill count |
| Magnani et al. [65] (2025), USA | RCT | Patients with AF (N=243; EG=123, CG=120) | Smartphone app with a relational agent for education, adherence monitoring, self-care, and heart rate and rhythm monitoring | 48 | Active comparator | PDC |
| Mehta et al. [66] (2024), USA | RCT | Patients with hypertension (N=86; EG1=35, EG2=36, CG=15) | Bidirectional SMS monitoring | 12 | Usual care | Self-reported MA |
| Meyer et al. [67] (2025), Germany | RCT | Patients with hypertension (N=102; EG=52, CG=50) | Internet-based cognitive behavioral therapy, lifestyle counseling, and self-monitoring | 12 | Usual care | RAI |
| Morawski et al. [68] (2018), USA | RCT | Patients with uncontrolled hypertension (N=411; EG=209, CG=202) | Medisafe smartphone app | 12 | Usual care | MMAS-8 |
| Ni et al. [69] (2018), China | RCT | Patients with CHD (N=50; EG=25, CG=25) | Text messages (education via WeChat and medication reminders) | 4 | Usual care | VES |
| Ni et al. [70] (2022), China | RCT | Patients with CHD (N=196; EG=103, CG=93) | Messaging intervention (reminders and education) | 9 | Usual care | VES |
| Park et al. [71] (2015), USA | RCT | Patients with CHD (N=90; EG1=30, EG2=30, CG=30) | SMS reminders and education (EG1) vs. SMS (education only) | 4 | No intervention | MMAS-8 |
| Persell et al. [72] (2020), USA | RCT | Participant with uncontrolled hypertension (N=333; EG=166, CG=167) | Smartphone coaching app with home BP monitoring | 24 | Active comparator | Self-reported MA |
| Santo et al. [73] (2019), Australia | RCT | Patients with CHD (N=163; EG=107, CG=56) | Medication reminder smartphone apps | 12 | Usual care | MMAS-8 |
| Schwalm et al. [74] (2019), Colombia and Malaysia | Cluster RCT | Patients with hypertension (N=1,371; EG=740, CG=631) | Tablet-based management algorithm, counselling, and adherence support | 48 | Usual care | MMAS-8 |
| Shi et al. [75] (2025), China | RCT | Patients with AF (N=208, EG=104, CG=104) | Digital animation-based education | 12 | Standard care | MARS-5 |
| Still et al. [76] (2020), USA | RCT | African Americans with hypertension (N=60; EG=30, CG=30) | Community and technology-based hypertension self-management | 12 | Usual care | HBCS |
| Ullrich et al. [77] (2025), Germany | RCT | Patients with CAD (N=240; EG=121, CG=119) | PreventiPlaque app for lifestyle change and adherence support | 48 | Standard care | Self-assessment of MA |
| Varleta et al. [78] (2017), Chile | RCT | Patients with hypertension (N=314; EG=163, CG=151) | SMS (education for medication adherence) | 24 | No intervention | MGL |
| Xu et al. [79] (2024), China | RCT | Patients with AF (N=96; EG=48, CG=48) | Alfalfa app for comprehensive AF management | 12 | Standard care | MMAS-8 |
| Yang et al. [80] (2023), China | RCT | Patients with hypertension (N=368; EG=184, CG=184) | Transitional care with WeChat support, telephone follow-up, and home visits | 52 | Usual care | Self-designed questionnaire |
| Yildirim Keskin et al. [81] (2025), Turkey | RCT | Patients with hypertension (N=80; EG=40, CG=40) | Mobile app with self-monitoring, medication reminders, education, and feedback | 5 | Standard care | HBCS |
| Yoon et al. [82] (2024), South Korea | RCT | Patients with AF (N=498; EG=248, CG=250) | App-based feedback for edoxaban adherence support | 24 | Standard care | Pill count |
| Yoon et al. [83] (2025), South Korea | RCT | Patients with uncontrolled hypertension (N=154; EG=79, CG=75) | BP self-monitoring app with feedback | 24 | Active comparator | Pill count |
| Zhai et al. [84] (2020), China | Cluster RCT | Patients with hypertension (N=384; EG=192, CG=192) | SMS and personal consultation | 12 | Usual care | MMAS-8 |
Table 1. Descriptive summary of the included studies (N=52)
CVD, cardiovascular disease; RCT, randomized controlled trial. a)Other countries include Jordan, Pakistan, Colombia, Nepal, South Africa, Brazil, Spain, Belgium, Canada, Iran, Taiwan, Palestine, Malaysia, Germany, Chile, and Turkey, as well as one multinational study. b)Others include cluster RCTs, crossover RCTs, and mixed-methods RCTs. c)Mixed or general CVD includes general CVD and combined conditions such as acute coronary syndrome, heart failure, or mechanical valve replacement.
Table 2. Characteristics of studies included in the systematic review (N=52)
ACS, acute coronary syndrome; AF, atrial fibrillation; Apps, applications; ARMS-14, adherence to refills and medication scale; BAQ, Brilique Adherence Questionnaire; BMQ, Brief Medication Questionnaire; BP, blood pressure; CAD, coronary artery disease; CG, control group; CHD, coronary heart disease; CHF, chronic heart failure; CVD, cardiovascular disease; EG, experimental group; HBCS, Hill-Bone Compliance Scale; HF, heart failure; MA, medication adherence; MAQ, Medication Adherence Questionnaire; MARS, Medication Adherence Rating Scale; MEMS, medication event monitoring system; MGL, Morisky-Green-Levine; MMAS, Morisky Medication Adherence Scale; MMAS-8, Morisky Medication Adherence Scale-8; MMS, Modified Morisky Scale; N, total sample size; PDC, proportion of days covered; RAI, Rief Adherence Index; RCT, randomized controlled trial; SMS, short message service; VES, Voils Medication Non-Adherence Extent Scale.

