 Submit an article
Submit an article
Articles
- Page Path
- HOME > J Korean Acad Nurs > Volume 56(1); 2026 > Article
-
Research Paper
외상 간호사 역량 강화를 위한 Trauma-nursing Education and Skill Support 프로그램 개발 및 검증: 유사실험연구 -
양태영1
 , 장명진2, 김기웅3, 소민4, 최미나5, 이은정6, 조진수5, 이지윤7, 임광균8, 김경미9, 백해준8, 왕선호10, 최진오11
, 장명진2, 김기웅3, 소민4, 최미나5, 이은정6, 조진수5, 이지윤7, 임광균8, 김경미9, 백해준8, 왕선호10, 최진오11 - Development and evaluation of the Trauma-nursing Education and Skill Support program to enhance trauma nursing competencies: a quasi-experimental study
-
Tae Yeong Yang1, Myung Jin Jang2, Ki Ung Kim3, Min So4, Mi Na Choi5, Eun Jung Lee6, Jin Su Jo5, Ji Yun Lee7, Kwang Kyun Lim8, Kyoung Mi Kim9, Hae Jun Baek8, Sun Ho Wang10, Jin Oh Choi11
-
Journal of Korean Academy of Nursing 2026;56(1):67-80.
DOI: https://doi.org/10.4040/jkan.25134
Published online: February 24, 2026
1동국대학교 WISE캠퍼스 간호대학 간호학과
2가천대 길병원 권역외상센터
3국군수도병원 국군외상센터
4원주세브란스기독병원 간호본부
5가톨릭대학교 의정부성모병원 간호본부
6국립중앙의료원 서울권역외상센터
7제주한라병원 권역외상센터
8충북대학교병원 권역외상센터
9단국대학교병원 권역외상센터
10강북삼성병원 간호본부
11아주대학교병원 간호본부
1Department of Nursing, College of Nursing, Dongguk University-WISE, Gyeongju, South Korea
2Regional Trauma Center, Gachon University Gil Medical Center, Incheon, South Korea
3Armed Forces Trauma Center, Korean Armed Forces Capital Hospital, Seongnam, South Korea
4Department of Nursing, Wonju Severance Christian Hospital, Wonju, South Korea
5Department of Nursing, Uijeongbu St. Mary's Hospital, The Catholic University of Korea, Uijeongbu, South Korea
6Regional Trauma Center, National Medical Center, Seoul, South Korea
7Regional Trauma Center, Cheju Halla General Hospital, Jeju, South Korea
8Regional Trauma Center, Chungbuk National University Hospital, Cheongju, South Korea
9Department of Nursing, Dankook National University, Cheonan, South Korea
10Department of Nursing, Kanbuk Samsung Hospital, Seoul, South Korea
11Department of Nursing, Ajou University Hospital, Suwon, South Korea
- Corresponding author: Myung Jin Jang Regional Trauma Center, Gachon University Gil Medical Center, 21 Namdong-daero 774beon-gil, Namdong-gu, Incheon 21565, South Korea E-mail: saguri5919@gilhospital.com
• Received: September 23, 2025 • Revised: December 26, 2025 • Accepted: December 27, 2025
© 2026 Korean Society of Nursing Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution NoDerivs License (http://creativecommons.org/licenses/by-nd/4.0) If the original work is properly cited and retained without any modification or reproduction, it can be used and re-distributed in any format and medium.
- 2,128 Views
- 275 Download
Abstract
-
Purpose
- This study aimed to develop and evaluate the effectiveness of the Trauma-nursing Education and Skill Support (TESS) program based on the ADDIE model (Analysis, Design, Development, Implementation, Evaluation model). The program was designed to enhance trauma nurses’ clinical competencies, including trauma-related knowledge, self-efficacy, and problem-solving ability, through the integration of theoretical education and simulation-based practice.
-
Methods
- A quasi-experimental study using a non-equivalent control group pretest–posttest design was conducted. Participants included 108 trauma nurses from regional trauma centers, military trauma centers, and emergency care facilities, who were assigned to an experimental group (n=52) or a control group (n=56). The TESS program consisted of a 2-day, 14-hour blended-learning course that included eight lecture sessions and four simulation-based practice stations. Data were collected at baseline, immediately after the intervention, and at 6 months using validated instruments measuring trauma-related knowledge, self-efficacy, and problem-solving ability. Two-way repeated-measures analysis of variance was used for data analysis.
-
Results
- The experimental group demonstrated significant improvements in trauma-related knowledge, self-efficacy, and problem-solving ability compared with baseline (all p<.001). These improvements were sustained at 6 months, although trauma-related knowledge scores showed a slight decline compared with immediate posttest levels. Between-group analyses confirmed significant group-by-time interaction effects for all outcomes: trauma-related knowledge (η2=0.12, p<.001), self-efficacy (η2=0.09, p=.002), and problem-solving ability (η2=0.08, p=.003).
-
Conclusion
- The TESS program effectively enhanced trauma nurses’ trauma-related knowledge, self-efficacy, and problem-solving ability, with effects sustained for up to 6 months. Incorporating blended learning and simulation-based training into standardized trauma nursing education may strengthen clinical competencies and ultimately contribute to improved patient outcomes.
서론
방법
1) 외상 지식
2) 자기효능감
3) 외상 간호 문제 해결능력
1) TESS 프로그램 개발
2) TESS 프로그램 효과 검증
결과
고찰
결론
-
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
-
Acknowledgements
The authors would like to express their sincere appreciation to the Korean Association for Nurses of Trauma (KANT) for their support in the operation of the TESS course and their assistance in facilitating this research.
-
Funding
This research received no external funding.
-
Data Sharing Statement
Please contact the corresponding author for data availability.
-
Author Contributions
Conceptualization or/and Methodology: TYY, MJJ, KUK. Data curation or/and Analysis: MJJ, KUK. Investigation: MS, MNC, EJL, JSJ, JYL, KKL, KMK, HJB, SHW, JNC. Project administration or/and Supervision: MJJ, KUK, JYL. Validation: TYY, MJJ. Visualization: TYY, MJJ. Writing: original draft or/and Review & Editing: TYY, MJJ. Final approval of the manuscript: all authors.
Article Information
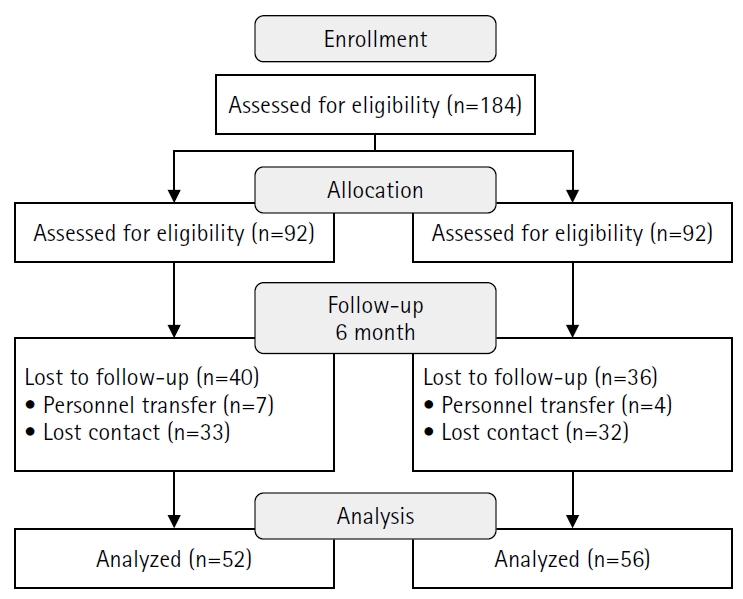
Table 1.Structure and components of the TESS program
AIS, Abbreviated Injury Scale; ISS, Injury Severity Score; CT, computed tomography; DCR, damage control resuscitation; EVD, external ventricular drain; FAST, focused assessment with sonography for trauma; GCS, Glasgow Coma Scale; IO, intraosseous; KTDB, Korean Trauma Data Bank; REBOA, resuscitative endovascular balloon occlusion of the aorta; TESS, Trauma-nursing Education and Skill Support.
Table 2.General characteristics and baseline homogeneity between groups (N=108)
χ² and t-values indicate results of the chi-square test and independent t-test, respectively. Problem-solving, self-efficacy, knowledge, and self-confidence variables indicate baseline scores prior to intervention.
SD, standard deviation; BSN, Bachelor of Science in Nursing; CN, charge nurse; Con., control group; Exp., experimental group; MS, Master of Science; PA, physician assistant; RN, registered nurse.
Table 3.Comparison of problem-solving ability, self-efficacy, and trauma-related knowledge across pre-education, post-education, and 6-month follow-up period (N=52)
Table 4.Comparison of changes in problem-solving ability, self-efficacy, and trauma-related knowledge between groups at the 6-month follow-up (N=108)
- 1. World Health Organization. Injuries and violence [Internet]. World Health Organization; 2024 [cited 2025 Apr 28]. Available from: https://www.who.int/news-room/fact-sheets/detail/injuries-and-violence
- 2. Lee S, Kim J, Lee J, Bae W. A community-based study of severe trauma, death, and disability, from 2015 to 2020. Jugan Geongang Gwa Jilbyeong. 2023;16(26):837-851. https://doi.org/10.56786/PHWR.2023.16.26.2ArticlePubMedPMC
- 3. Baik D, Yi N, Han O, Kim Y. Trauma nursing competency in the emergency department: a concept analysis. BMJ Open. 2024;14(6):e079259. https://doi.org/10.1136/bmjopen-2023-079259ArticlePubMedPMC
- 4. Polovitch S, Muertos K, Burns A, Czerwinski A, Flemmer K, Rabon S. Trauma nurse leads in a level I trauma center: roles, responsibilities, and trauma performance improvement outcomes. J Trauma Nurs. 2019;26(2):99-103. https://doi.org/10.1097/JTN.0000000000000431Article
- 5. Kim DM, Seo EJ. Analysis of nursing interventions in trauma-bay at the regional trauma center for patients with severe thoracic injuries. J Korean Biol Nurs Sci. 2021;23(2):138-150. https://doi.org/10.7586/jkbns.2021.23.2.138Article
- 6. McLeod K, Owens L, Williamson F, Faulkner B, McLanders M. Queensland Trauma Education (QTE): an innovative simulation program that addresses the needs and barriers of interprofessional trauma care education across a complex landscape. Rural Remote Health. 2024;24(2):8851. https://doi.org/10.22605/RRH8851ArticlePubMed
- 7. Chowdhury S, Almarhabi M, Varghese B, Leenen L. Trauma resuscitation training: an evaluation of nurses’ knowledge. J Trauma Nurs. 2022;29(4):192-200. https://doi.org/10.1097/JTN.0000000000000661ArticlePubMed
- 8. Yustilawati E, Zahrani G, Fitriani A, Ria P, Hakim SA. Analysis of knowledge and nurse competencies related to advanced care for trauma patients in the emergency room in South Sulawesi. J Pendidik Keperawatan Indones. 2023;9(2):163-176. https://doi.org/10.17509/jpki.v9i2Article
- 9. Ancel G. Problem-solving training: effects on the problem-solving skills and self-efficacy of nursing students. Eurasian J Educ Res. 2016;16(64):231-246. https://doi.org/10.14689/ejer.2016.64.13Article
- 10. Kim H, Joe S, Hong E. Core competency of nurses at regional trauma centers in South Korea. Korean J Mil Nurs Res. 2018;36(2):29-40. https://doi.org/10.31148/kjmnr.2018.36.2.29Article
- 11. Knight C, Smith SR. Developing and evaluating a major trauma course and coaching programme for ward nurses. Emerg Nurse. 2024;32(5):26-33. https://doi.org/10.7748/en.2024.e2184ArticlePubMed
- 12. Kim HW, Roh YS. Perceived trauma nursing core competency, interprofessional collaborative competency, and associated barriers among regional trauma center nurses. Int Emerg Nurs. 2024;72:101388. https://doi.org/10.1016/j.ienj.2023.101388ArticlePubMed
- 13. Jung YJ, Kim S, Noh S, Seo E, Jung S, Kim J. Status and needs of continuing education for trauma nursing. J Trauma Inj. 2019;32(3):157-167. https://doi.org/10.20408/jti.2019.016Article
- 14. Cho SY, Seo YM, Jung EK, Choi JY. Educational needs assessment for nurses in the regional trauma centers. Korean J Mil Nurs Res. 2016;34(2):52-68. https://doi.org/10.31148/kjmnr.2016.34.2.52Article
- 15. Kim KM, Kim JK. A convergence study on education status, educational needs, and nursing competence of regional trauma intensive care unit nurses. J Korea Converg Soc. 2020;11(3):321-331. https://doi.org/10.15207/JKCS.2020.11.3.321Article
- 16. Muruganantham G. Developing of E-content package by using ADDIE model. Int J Appl Res. 2015;1(3):52-54.
- 17. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Routledge; 2013.
- 18. Polit DF, Beck CT. Nursing research: generating and assessing evidence for nursing practice. 8th ed. Lippincott Williams & Wilkins; 2008.
- 19. American College of Surgeons Committee on Trauma. Advanced Trauma Life Support (ATLS): student course manual. 10th ed. American College of Surgeons; 2018.
- 20. Emergency Nurses Association. Trauma Nursing Core Course (TNCC) provider manual. 8th ed. Jones & Bartlett Learning; 2019.
- 21. Sherer M, Maddux JE, Mercandante B, Prentice-Dunn S, Jacobs B, Rogers RW. The self-efficacy scale: construction and validation. Psychol Rep. 1982;51(2):663-671. https://doi.org/10.2466/pr0.1982.51.2.663Article
- 22. Lee GS. Relationships among job stress, resilience and self-efficacy in nurses [master’s thesis]. Nonsan: Konyang University; 2018.
- 23. Lee WS, Park SH, Choi EY. Development of a Korean problem solving process inventory for adults. J Korean Acad Fundam Nurs. 2008;15(4):548-557.
- 24. Lee HJ. Effects of convergence-based simulation education on the problem solving ability, self-efficacy and performance confidence of core fundamental nursing skills for nursing students. J Converg Inf Technol. 2020;10(1):44-50. https://doi.org/10.22156/CS4SMB.2020.10.01.044Article
- 25. Kim JA, Kim IA. The effect of class using case-based learning and inferential reading for nursing students. Korean J Educ Methodol Stud. 2022;34(4):857-872. https://doi.org/10.17927/tkjems.2022.34.4.857Article
- 26. Park IH, Hong JM, Shin S. Strategies of peer-assisted learning and their effectiveness in nursing education: a systematic review. Korean Med Educ Rev. 2016;18(2):106-113. https://doi.org/10.17496/KMER.2016.18.2.106Article
- 27. Song Y, Park S. Effectiveness of debriefing in simulation-based education for nursing students: a systematic review and meta-analysis. J Korean Acad Fundam Nurs. 2022;29(4):399-415. https://doi.org/10.7739/jkafn.2022.29.4.399Article
- 28. Yun J, Kang I. The effect of the debriefing method of simulation nursing practice education: a literature review. J Korea Acad Ind Coop Soc. 2022;23(10):593-604. https://doi.org/10.5762/KAIS.2022.23.10.593Article
- 29. Mohammad A, Branicki F, Abu-Zidan FM. Educational and clinical impact of Advanced Trauma Life Support (ATLS) courses: a systematic review. World J Surg. 2014;38(2):322-329. https://doi.org/10.1007/s00268-013-2294-0ArticlePubMed
- 30. Donker SC, Vorstenbosch MA, Gerhardus MJ, Thijssen DH. Retrieval practice and spaced learning: preventing loss of knowledge in Dutch medical sciences students in an ecologically valid setting. BMC Med Educ. 2022;22(1):65. https://doi.org/10.1186/s12909-021-03075-yArticlePubMedPMC
- 31. Gorman KM, Dumire RD. Knowledge retention of the traumatic brain injury guidelines at a Level 1 trauma center. J Emerg Crit Care Med. 2019;3:17. https://doi.org/10.21037/jeccm.2019.02.06Article
- 32. Subramaniam T, Hassan S, Tan AJ, Abdul Rahman SR. Impact of cardiac life support training on retention of knowledge measured by pretest, immediate posttest, and 6-months posttest. Int E-J Sci Med Educ. 2022;169(2):28-35. https://doi.org/10.56026/imu.16.2.28Article
- 33. Hilsmann N, Dodson C. Mobile microlearning in continuing professional development for nursing: a scoping review. J Contin Educ Nurs. 2025;56(2):53-62. https://doi.org/10.3928/00220124-20250121-05ArticlePubMed
- 34. Phillips JM, Feldman K, Miller PS, Galuska L. The impact of boost methodology on nurse knowledge retention: a longitudinal, quasi-experimental sepsis simulation pilot study. J Nurses Prof Dev. 2021;37(1):3-11. https://doi.org/10.1097/NND.0000000000000696ArticlePubMed
- 35. Benner P. From novice to expert: excellence and power in clinical nursing practice. Addison-Wesley; 1984.
- 36. Song YA. Effects of integrative simulation practice on nursing knowledge, critical thinking, problem-solving ability, and immersion in problem-based learning among nursing students. Korean J Women Health Nurs. 2020;26(1):61-71. https://doi.org/10.4069/kjwhn.2020.03.15.1ArticlePubMedPMC
- 37. Pu Y, Xie H, Fu L, Zhang X, Long T, Su X, et al. Self-efficacy as a mediator in the relationship between clinical learning environment and core nursing competence of intern nursing students: a multicentre cross-sectional study. BMJ Open. 2025;15(5):e094858. https://doi.org/10.1136/bmjopen-2024-094858ArticlePubMedPMC
- 38. Badakhshan R, Badakhshan S, Bagheriyeh F, Hosseinzadegan F. The relationship between self-directed learning ability and clinical competence among nursing students: a cross-sectional descriptive study. BMC Med Educ. 2025;25(1):1508. https://doi.org/10.1186/s12909-025-08108-4ArticlePubMedPMC
- 39. Alrashidi N, Pasay An E, Alrashedi MS, Alqarni AS, Gonzales F, Bassuni EM, et al. Effects of simulation in improving the self-confidence of student nurses in clinical practice: a systematic review. BMC Med Educ. 2023;23(1):815. https://doi.org/10.1186/s12909-023-04793-1ArticlePubMedPMC
- 40. Lasater K. High-fidelity simulation and the development of clinical judgment: students’ experiences. J Nurs Educ. 2007;46(6):269-276. https://doi.org/10.3928/01484834-20070601-06ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteDevelopment and evaluation of the Trauma-nursing Education and Skill Support program to enhance trauma nursing competencies: a quasi-experimental study
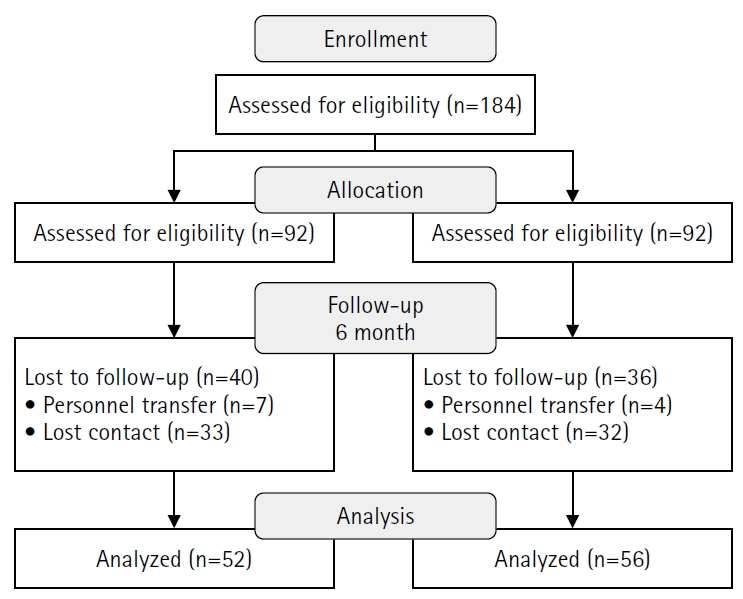
Fig. 1. Flow diagram of participant recruitment and retention.
Fig. 1.
Development and evaluation of the Trauma-nursing Education and Skill Support program to enhance trauma nursing competencies: a quasi-experimental study
| Session | Session title | Learning objectives and key content | Instructional strategies | Duration (min) |
|---|---|---|---|---|
| Lecture | ||||
| 1 | Trauma system | Understand the concept of trauma and the structure of the trauma system and explain the national-level trauma patient management system. | Presentation of Korean trauma statistics and key cases; hands-on practice calculating AIS and ISS scores. | 50 |
| • Definition of trauma | ||||
| • National and global trauma statistics | ||||
| • Role of regional trauma centers and transfer systems | ||||
| • Principles of AIS coding | ||||
| • ISS calculation | ||||
| • Case examples using KTDB | ||||
| 2 | Damage control resuscitation | Understand the concept and core principles of DCR and develop appropriate interventions for patients with massive hemorrhage. | Case analysis of hemorrhage management and problem-solving activities. | 50 |
| • Three pillars of DCR (hemorrhage control, hypothermia prevention, coagulopathy management) | ||||
| • Target blood pressure setting | ||||
| • Fluid restriction strategies | ||||
| • Hemostatic agent selection | ||||
| • Massive Transfusion Protocol | ||||
| 3 | Shock management | Understand the pathophysiology of various types of shock and establish priority nursing interventions based on the shock stage. | Case-based analysis of shock types and planning of priority nursing interventions. | 50 |
| • Pathophysiology and clinical signs of hypovolemic, cardiogenic, neurogenic, and septic shock | ||||
| • Initial assessment indicators (blood pressure, heart rate, skin response, etc.) | ||||
| • Interpretation of shock indices (Shock Index, lactate levels) | ||||
| • Nursing intervention protocols by shock type and severity | ||||
| 4 | Imaging for trauma | Understand the indications for imaging studies (X-ray, CT) in trauma patients and interpret key radiologic findings by injury site. | Practice interpreting lesion locations using diverse imaging materials and discuss indications for emergency interventions. | 50 |
| • Imaging protocols and positioning for FAST and chest/pelvis X-rays | ||||
| • Identification of critical findings in head, chest, and abdominal trauma via CT | ||||
| • Radiologic characteristics of pneumothorax and pelvic fractures | ||||
| 5 | Head trauma nursing | Understand the anatomical mechanisms, clinical manifestations, and treatment principles of head trauma, and apply appropriate nursing interventions. | Analyze cases involving altered consciousness, practice GCS application, and EVD management procedures. | 50 |
| • Major anatomical structures of the brain | ||||
| • Classification of head trauma (epidural hematoma, subdural hematoma, subarachnoid hemorrhage) | ||||
| • GCS assessment | ||||
| • EVD management and nursing care | ||||
| 6 | Spine trauma nursing | Understand the classification of spinal injuries, segment-specific symptoms, and procedures for immobilization and transport, and apply them in clinical practice. | Case-based learning using patients with spinal cord injuries to analyze injury level and appropriate care strategies. | 50 |
| • Characteristics of cervical, thoracic, and lumbar spine injuries | ||||
| • Spine precautions | ||||
| • Application of cervical collar (C-collar) | ||||
| • Log-roll technique | ||||
| • Long spine board transport standards | ||||
| 7 | Thoracic trauma nursing | Understand the pathophysiology of thoracic trauma and emergency management procedures and accurately perform nursing care related to chest tube insertion. | Case studies on thoracic trauma and guided learning of chest tube insertion procedures. | 50 |
| • Pathophysiology of flail chest, hemothorax, and pneumothorax | ||||
| • Indications and anatomical sites for chest tube insertion | ||||
| • Management of drainage systems | ||||
| 8 | Abdomen-pelvic trauma nursing | Understand the symptoms and diagnostic approaches for abdominal and pelvic trauma and establish priorities for nursing interventions. | Case analysis of abdominal pain, hands-on practice for hemorrhage control in pelvic fractures, and interpretation of FAST imaging. | 50 |
| • Differences between solid and hollow organ injuries | ||||
| • Focused Assessment with Sonography for Trauma | ||||
| • Characteristics of pelvic fractures | ||||
| • Identification of bleeding signs and nursing care priorities | ||||
| Simulation | ||||
| 1 | Hemorrhage control & nursing | Understand the indications for REBOA in patients with massive hemorrhage and the nurse’s role in preparation and monitoring during the procedure. | Hands-on practice with REBOA setup and procedure flow, balloon zone identification, and simulation-based patient monitoring. | 60 |
| • REBOA procedural steps (insertion, inflation, deflation) | ||||
| • Effectiveness depending on balloon zone placement | ||||
| • Key indicators for hemorrhage monitoring | ||||
| 2 | Immobilization nursing | Learn the types and application methods of immobilization devices used in trauma patient transport and stabilization and apply them in clinical scenarios. | Simulation of device application and removal, scenario-based practice for pelvic binder application. | 60 |
| • Indications and usage of cervical collars, Kendrick Extrication Device, and pelvic binders | ||||
| 3 | Nursing intervention for trauma patients I | Enhance nurses’ problem-solving skills and clinical decision-making through simulation of diverse trauma scenarios. | Team-based scenario response, problem identification, and intervention prioritization, debriefing with structured feedback. | 60 |
| Simulation case 1: Multiple trauma involving shock and head injury | ||||
| 4 | Nursing intervention for trauma patients II | Train nursing interventions and multidisciplinary collaboration in complex trauma situations. | Scenario-based communication and collaboration exercises, evaluation of nursing interventions, and role-specific feedback. | 60 |
| Simulation case 2: Multiple trauma involving thoracic injury and abdominal bleeding | ||||
| 5 | Catheterization management | Understand the indications and insertion procedures for catheter and IO devices, and practice methods for verifying placement and providing nursing care. | Practice IO insertion, verify placement using X-ray images, and simulate post-insertion monitoring and infection prevention care. | 60 |
| • Urinary catheterization | ||||
| • Indications and anatomical sites for IO insertion | ||||
| • Imaging-based confirmation of device placement |
| Characteristic | Mean±SD or n (%) | χ2 or t (p) | ||
|---|---|---|---|---|
| Total (N=108) | Exp. (n=52) | Con. (n=56) | ||
| Age (yr) | 29.7±4.30 | 29.5±4.15 | 30.0±4.46 | –0.63 (.532) |
| Gender | 4.44 (.035) | |||
| Male | 22 (20.4) | 15 (28.8) | 7 (12.5) | |
| Female | 86 (79.6) | 37 (71.2) | 49 (87.5) | |
| Total clinical experience (mo) | 71.72±44.26 | 69.60±39.61 | 73.73±48.53 | –0.48 (.632) |
| Trauma center experience (mo) | 35.90±30.36 | 30.56±31.10 | 40.95±29.02 | –1.79 (.077) |
| Position | 4.45 (.108) | |||
| RN | 81 (75.0) | 40 (76.9) | 41 (73.2) | |
| CN | 19 (17.6) | 6 (11.5) | 13 (23.2) | |
| PA | 8 (7.4) | 6 (11.5) | 2 (3.6) | |
| Level of education | 5.99 (.050) | |||
| College | 4 (3.7) | 3 (5.8) | 1 (1.8) | |
| BSN | 94 (87.0) | 41 (78.8) | 53 (94.6) | |
| MS | 10 (9.3) | 8 (15.4) | 2 (3.6) | |
| Problem-solving ability | 111.98±3.97 | 111.43±3.06 | 0.21 (.832) | |
| Self-efficacy | 56.48±9.66 | 58.66±7.22 | –1.33 (.185) | |
| Trauma-related knowledge | 61.25±14.10 | 66.43±14.04 | –1.91 (.059) | |
| Variable | Mean±SD or n (%) | η2 | F | p | MD (p) | |||
|---|---|---|---|---|---|---|---|---|
| Pre-education | Post-education | 6-mo follow-up | Pre vs. Post | Post vs. 6 mo | ||||
| Problem solving ability | 111.98±13.97 | 117.37±14.18 | 117.48±15.52 | 0.11 | 6.11 | .003 | 5.39 (.008) | 0.11 (.958) |
| Self-efficacy | 56.48±9.66 | 62.08±7.85 | 61.83±8.36 | 0.17 | 10.29 | <.001 | 5.60 (<.001) | –0.25 (.825) |
| Trauma-related knowledge | 61.25±14.10 | 84.13±10.65 | 76.15±11.66 | 0.65 | 94.35 | <.001 | 22.88 (<.001) | –7.98 (<.001) |
| Variable | Groups | Pre-test | 6-mo follow-up | Source | η2 | F | p |
|---|---|---|---|---|---|---|---|
| Problem solving ability | Exp. | MD=5.50, p=.010 | Group | 3.03 | .085 | ||
| 111.98±13.97 | 117.48±15.52 | Time | 2.16 | .145 | |||
| Con. | MD=–1.88, p=.306 | Group*Time | 0.08 | 8.93 | .003 | ||
| 111.43±13.06 | 109.55±14.13 | ||||||
| Self-efficacy | Exp. | MD=5.35, p<.001 | Group | 0.15 | .701 | ||
| 56.48±9.66 | 61.83±8.36 | Time | 9.79 | .002 | |||
| Con. | MD=–0.05, p=.960 | Group*Time | 0.09 | 10.19 | .002 | ||
| 58.66±7.22 | 58.61±7.76 | ||||||
| Trauma-related knowledge | Exp. | MD=8.30, p<.001 | Group | 0.00 | .968 | ||
| 61.25±14.10 | 76.15±11.66 | Time | 54.43 | <.001 | |||
| Con. | MD=2.4, p=.020 | Group*Time | 0.12 | 14.61 | <.001 | ||
| 66.43±14.04 | 71.16±15.46 |
Table 1. Structure and components of the TESS program
AIS, Abbreviated Injury Scale; ISS, Injury Severity Score; CT, computed tomography; DCR, damage control resuscitation; EVD, external ventricular drain; FAST, focused assessment with sonography for trauma; GCS, Glasgow Coma Scale; IO, intraosseous; KTDB, Korean Trauma Data Bank; REBOA, resuscitative endovascular balloon occlusion of the aorta; TESS, Trauma-nursing Education and Skill Support.
Table 2. General characteristics and baseline homogeneity between groups (N=108)
χ² and t-values indicate results of the chi-square test and independent t-test, respectively. Problem-solving, self-efficacy, knowledge, and self-confidence variables indicate baseline scores prior to intervention. SD, standard deviation; BSN, Bachelor of Science in Nursing; CN, charge nurse; Con., control group; Exp., experimental group; MS, Master of Science; PA, physician assistant; RN, registered nurse.
Table 3. Comparison of problem-solving ability, self-efficacy, and trauma-related knowledge across pre-education, post-education, and 6-month follow-up period (N=52)
SD, standard deviation; F, F statistic from repeated measures analysis of variance; MD, mean difference; η2, partial eta squared.
Table 4. Comparison of changes in problem-solving ability, self-efficacy, and trauma-related knowledge between groups at the 6-month follow-up (N=108)
Values are presented as mean±standard deviation unless otherwise stated. Con., control group; Exp., experimental group; F, F statistic from two-way repeated measures analysis of variance; MD, mean difference; η2, partial eta squared.

